Forehead Brow Bone and Temporal Contouring
Forehead Brow Bone and Temporal Contouring
Are you unsatisfied by the shape of your forehead or the appearance of your brow bones? Dr. Barry Eppley, is a international specialist in the many types of forehead and brow bone contouring surgeries.
AESTHETIC UNITS OF THE FOREHEAD
 The forehead is a major part of the face and occupies up to one-third of its total surface area. It is a major contributor to facial aesthetics even though it has only one obvious feature: the eyebrows. However, the forehead actually has three features that create the visual impression of its overall size. The top of the forehead is marked by the variable position of the frontal hairline, which differs greatly between males and females. The bottom of the forehead is outlined by the eyebrows and the brow bones, which are the ridges of skull bone just above the eyes. The sides of the forehead are defined by the temporal ridges, the edges of the bony forehead where it meets with the large temporalis muscles.
The forehead is a major part of the face and occupies up to one-third of its total surface area. It is a major contributor to facial aesthetics even though it has only one obvious feature: the eyebrows. However, the forehead actually has three features that create the visual impression of its overall size. The top of the forehead is marked by the variable position of the frontal hairline, which differs greatly between males and females. The bottom of the forehead is outlined by the eyebrows and the brow bones, which are the ridges of skull bone just above the eyes. The sides of the forehead are defined by the temporal ridges, the edges of the bony forehead where it meets with the large temporalis muscles.
MALE vs FOREHEAD SHAPE
 The shape of the bony forehead (amount of convexity) and the prominence of the brow ridges help define the masculine or feminine appearance. A long forehead is more acceptable in a male because of the variability of the frontal hairline. The bone ridge running across the forehead above the eyes, known as brow bossing (supraorbital rims), is more pronounced in males. The degree of acceptable brow protrusion is not well-defined and can certainly become excessive, thereby causing an over-masculine or Neanderthal appearance. Male brow protrusion should be enough to create a noticeable break between the brow ridge and the forehead bone above it. It may also extend off to the side, tapering down onto the lateral orbital rims.
The shape of the bony forehead (amount of convexity) and the prominence of the brow ridges help define the masculine or feminine appearance. A long forehead is more acceptable in a male because of the variability of the frontal hairline. The bone ridge running across the forehead above the eyes, known as brow bossing (supraorbital rims), is more pronounced in males. The degree of acceptable brow protrusion is not well-defined and can certainly become excessive, thereby causing an over-masculine or Neanderthal appearance. Male brow protrusion should be enough to create a noticeable break between the brow ridge and the forehead bone above it. It may also extend off to the side, tapering down onto the lateral orbital rims.
 Females have almost no discernible brow bossing because their foreheads are more rounded with a fairly flat front. In profile, female foreheads are more vertical instead of backward sloping. This means that some brow bossing may be aesthetically acceptable when there is no break between the brow ridge and vertical forehead bone above it; it should flow smoothly without a noticeable transition. The amount of convexity in profile view, however, is important; it should not stick out further than the lowest edge of the brow ridge. The sides of the brow ridges are also more tapered towards the temples, unlike in males, in which the sides can be more boxy or square-shaped.
Females have almost no discernible brow bossing because their foreheads are more rounded with a fairly flat front. In profile, female foreheads are more vertical instead of backward sloping. This means that some brow bossing may be aesthetically acceptable when there is no break between the brow ridge and vertical forehead bone above it; it should flow smoothly without a noticeable transition. The amount of convexity in profile view, however, is important; it should not stick out further than the lowest edge of the brow ridge. The sides of the brow ridges are also more tapered towards the temples, unlike in males, in which the sides can be more boxy or square-shaped.
BROW BONE REDUCTION


![]()
![]() Brow bone reduction is done in three types of patients, the cis-male with large hypertrophic frontal sinuses/brow bone protrusions, the transgender male to female patient and the cis-female with either central or lateral brow bone protrusions. Most male and transgender brow bone reductions require a bone flap removal, reshaping and setback technique for the most visible reduction. Infrequently, burring reduction alone may be sufficient but only if the frontal sinuses are underdeveloped or have failed to develop at all. The relatively thin outer layer of bone overlying the frontal sinus precludes burring reduction for most patients.
Brow bone reduction is done in three types of patients, the cis-male with large hypertrophic frontal sinuses/brow bone protrusions, the transgender male to female patient and the cis-female with either central or lateral brow bone protrusions. Most male and transgender brow bone reductions require a bone flap removal, reshaping and setback technique for the most visible reduction. Infrequently, burring reduction alone may be sufficient but only if the frontal sinuses are underdeveloped or have failed to develop at all. The relatively thin outer layer of bone overlying the frontal sinus precludes burring reduction for most patients.
One important consideration in any brow bone reduction is the slope of the forehead above it. If the slope of the forehead is too far backward the addition of forehead augmentation at the same time as brow bone reduction can provide an optimal forehead reshaping effect.
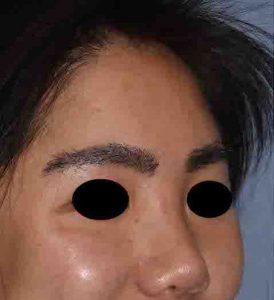
![]() One unique type of brow bone reduction is that when only the tail of the brow needs to be reduced. This may be needed in transgender brow bone reduction patients where the tail of the brow bone has been neglected in the initial surgery or in the cis-female who has a prominent outer brow bone that sticks out below the tail of the eyebrow. It can also be part of Cat Eye surgery to help get an accentuated temporal browlift effect. This is the one type of brow bone reduction that can be done through an upper eyelid incision and is called a transpalpebral brow bone reduction.
One unique type of brow bone reduction is that when only the tail of the brow needs to be reduced. This may be needed in transgender brow bone reduction patients where the tail of the brow bone has been neglected in the initial surgery or in the cis-female who has a prominent outer brow bone that sticks out below the tail of the eyebrow. It can also be part of Cat Eye surgery to help get an accentuated temporal browlift effect. This is the one type of brow bone reduction that can be done through an upper eyelid incision and is called a transpalpebral brow bone reduction.
BROW BONE AUGMENTATION
Augmentation of the brows has historically been done using various implant materials, most commonly that of bone cements. (PMMA acrylic and HA hydroxyapatite cement). Besides the limited detailed shaping that these materials allow they also require an open placement technique which for many men is a major aesthetic liability.

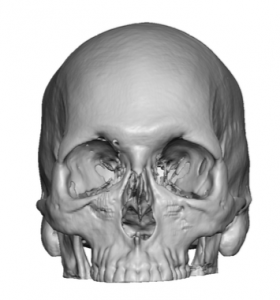
 The contemporary approach to brow bone augmentation is the creation of a custom brow bone implant made from the patient’s 3D CT scan. This allows a precise design to be made before surgery which has the optimal brow bone shape. It can also be placed through a very limited scalp incision using an endoscopic technique. Depending upon how far down along the lateral orbital rim the implant design goes it may need to be supplemented with small upper eyelid incisions for assured positioning.
The contemporary approach to brow bone augmentation is the creation of a custom brow bone implant made from the patient’s 3D CT scan. This allows a precise design to be made before surgery which has the optimal brow bone shape. It can also be placed through a very limited scalp incision using an endoscopic technique. Depending upon how far down along the lateral orbital rim the implant design goes it may need to be supplemented with small upper eyelid incisions for assured positioning.
FOREHEAD REDUCTION
Hairline Advancement

 The length of the forehead can also be reduced both in its bony bulging and in its forehead skin length. Through a frontal hairline (pretrichial) incision, the frontal hairline/scalp can be brought forward and excess vertical length of forehead skin removed. This shortens the long forehead and puts the scalp in a more aesthetic position. In less common cases, a staged approach with a tissue expander may be used when the hairline needs to come forward more than 1.5 to 2 cms. Through a hairline incision, forehead bulging can be shaved down to reduce a small amount of excessive convexity and forehead width. Often this is done at the same time as a hairline advancement/lowering.
The length of the forehead can also be reduced both in its bony bulging and in its forehead skin length. Through a frontal hairline (pretrichial) incision, the frontal hairline/scalp can be brought forward and excess vertical length of forehead skin removed. This shortens the long forehead and puts the scalp in a more aesthetic position. In less common cases, a staged approach with a tissue expander may be used when the hairline needs to come forward more than 1.5 to 2 cms. Through a hairline incision, forehead bulging can be shaved down to reduce a small amount of excessive convexity and forehead width. Often this is done at the same time as a hairline advancement/lowering.
Bony Forehead Reduction/Contouring
Frontal Bossing Reduction

 The frontal bone of the forehead can also be modified to reduce its projection and width. Using a bone burring or shaving technique the outer cortical layer can be removed to create less frontal projection (frontal bossing reduction) as well as a change in width. (reduction of the bony temporal lines) Like all forms of skull reduction the amount reduction is controlled by how much of the skull’s thickness can be safely removed.
The frontal bone of the forehead can also be modified to reduce its projection and width. Using a bone burring or shaving technique the outer cortical layer can be removed to create less frontal projection (frontal bossing reduction) as well as a change in width. (reduction of the bony temporal lines) Like all forms of skull reduction the amount reduction is controlled by how much of the skull’s thickness can be safely removed.
Combination Frontal Bossing Reduction with Hairline Advancement

 It is not uncommon to combine both forms of forehead reduction as high hairlines are often associated with some degree of frontal bossing. Given that a pretrichial incision is needed for the frontal hairline advancement this provides an opportunity for forehead bone reshaping as well.
It is not uncommon to combine both forms of forehead reduction as high hairlines are often associated with some degree of frontal bossing. Given that a pretrichial incision is needed for the frontal hairline advancement this provides an opportunity for forehead bone reshaping as well.
Forehead Osteoma Removal

 One discrete form of bony forehead reduction is the common osteoma. This is a small raised circular area of bone that can occur anywhere on the forehead. It is most commonly associated with a prior history of trauma which can stimulate bone formation from the bruise at the subperiosteal level. Although they are an equal number of forehead osteomas where the patient can no recall any history of forehead trauma. Forehead osteomas are usually removed by either a small hairline incision in line directly above it or using a scalp-based endoscopic technique.
One discrete form of bony forehead reduction is the common osteoma. This is a small raised circular area of bone that can occur anywhere on the forehead. It is most commonly associated with a prior history of trauma which can stimulate bone formation from the bruise at the subperiosteal level. Although they are an equal number of forehead osteomas where the patient can no recall any history of forehead trauma. Forehead osteomas are usually removed by either a small hairline incision in line directly above it or using a scalp-based endoscopic technique.
Forehead Eminence (Horn) Reduction

 A discrete type of bone formation on the forehead, often confused with an osteoma, are forehead horns. These are small rounded bony prominences in the upper forehead that usually paired. They are technically known as frontal eminences which are a normal part of the forehead development. They can be more prominent in some and are especially noticeable in certain lighting. They can occur as a paired rounded prominences or can be connected for a more ‘dogbone’ appearance. Forehead horns and dogbones can be reduced by a bone burring technique through small hairline incisions.
A discrete type of bone formation on the forehead, often confused with an osteoma, are forehead horns. These are small rounded bony prominences in the upper forehead that usually paired. They are technically known as frontal eminences which are a normal part of the forehead development. They can be more prominent in some and are especially noticeable in certain lighting. They can occur as a paired rounded prominences or can be connected for a more ‘dogbone’ appearance. Forehead horns and dogbones can be reduced by a bone burring technique through small hairline incisions.
FOREHEAD AUGMENTATION
 Augmentation of the forehead can be done using different types of materials. Historically, and still occasionally used, is the application of different types of bone cements. PMMA (polymethylmethacrylate) and HA (hydroxyapatite) are the two basic types of bone cements used in forehead augmentation. Their use is limited by the need for wide open access for placement (full coronal scalp incision), the need for intraoperative shaping of putty-like materials until they cure and the inability to cross the bony temporal line unto the fascia.
Augmentation of the forehead can be done using different types of materials. Historically, and still occasionally used, is the application of different types of bone cements. PMMA (polymethylmethacrylate) and HA (hydroxyapatite) are the two basic types of bone cements used in forehead augmentation. Their use is limited by the need for wide open access for placement (full coronal scalp incision), the need for intraoperative shaping of putty-like materials until they cure and the inability to cross the bony temporal line unto the fascia.
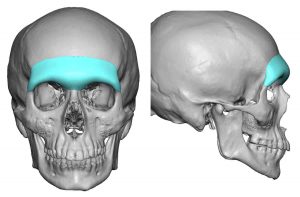
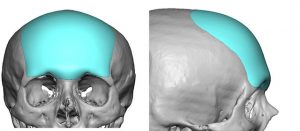 The contemporary method of forehead augmentation is a custom implant made from the patient’s 3D CT scan. The ability to create a thoughtful implant design before surgery allows for the best shape of the forehead possible. Such forehead implant designs can include the brow bone area as well if desired. (which is common in male forehead augmentations)
The contemporary method of forehead augmentation is a custom implant made from the patient’s 3D CT scan. The ability to create a thoughtful implant design before surgery allows for the best shape of the forehead possible. Such forehead implant designs can include the brow bone area as well if desired. (which is common in male forehead augmentations)
 One of the very important benefits of a custom forehead implant is the ability to place it through a small scalp incision. Between the preoperative design and the ability to allow the implant to go through a limited scalp incision makes the custom implant the superior forehead augmentation method today.
One of the very important benefits of a custom forehead implant is the ability to place it through a small scalp incision. Between the preoperative design and the ability to allow the implant to go through a limited scalp incision makes the custom implant the superior forehead augmentation method today.
AESTHETIC TEMPORAL CONTOURING
While the temporal region initially may not be thought of as part of the forehead, many patients when talking about their foreheads may also reference the temples. The temples is often perceived as the side of the forehead and for some patients is an important consideration with the forehead or as a standard alone treatment area.
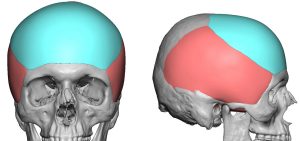
 The temporal region is anatomically the entire size of the head which begins at the bony temporal lines of the forehead and extends all the way to the back of the head. The extent that the temporal region covers can be easily seen in a skull by tracing the outline of the bony temporal line from the forehead to the back of the head. From an aesthetic standpoint it is best to think of the temporal region as having two main zones. The anterior temporal area is by the side of the eye and the non-hair bearing region that extends back into the hairline. The posterior temporal region is almost the entire hair bearing area along the side of the head. While the temporal muscle is not really divided into such anterior and posterior zones to is a good way to the about surgery used to either enlarge or reduce its size.
The temporal region is anatomically the entire size of the head which begins at the bony temporal lines of the forehead and extends all the way to the back of the head. The extent that the temporal region covers can be easily seen in a skull by tracing the outline of the bony temporal line from the forehead to the back of the head. From an aesthetic standpoint it is best to think of the temporal region as having two main zones. The anterior temporal area is by the side of the eye and the non-hair bearing region that extends back into the hairline. The posterior temporal region is almost the entire hair bearing area along the side of the head. While the temporal muscle is not really divided into such anterior and posterior zones to is a good way to the about surgery used to either enlarge or reduce its size.
TEMPORAL REDUCTION
When the temporal area bulges out (increased convexity) or the sides of the head (above the ears) are too wide, the posterior temporal muscle is either part or completely the cause of it. It is a common misconception that it is a bone problem due to an understandable lack of appreciation and how large and thick the temporalis muscle is over this area on the side of the skull. While in some cases the undesired widening or thickness of the muscle may be in both the anterior and posterior zone, most commonly it is limited to the side of the head and not by the side of the eye. The definitive test as whether this is a muscle-based head convexity is if one opens their mouth as wide as possible and the convexity above the ear flattens to an acceptable width.



 Temporal muscle reduction can be effectively done with Botox injections. But the dosage is high, the amount of muscle shrinkage is not always predictable and its effects will be short term. Temporal muscle reduction surgery is the most effective approach and is done by removing the entire posterior section of the muscle from an incision behind the ear. This causes no functional issues with mouth opening or closing.
Temporal muscle reduction can be effectively done with Botox injections. But the dosage is high, the amount of muscle shrinkage is not always predictable and its effects will be short term. Temporal muscle reduction surgery is the most effective approach and is done by removing the entire posterior section of the muscle from an incision behind the ear. This causes no functional issues with mouth opening or closing.
The anterior temporal muscle can be reduced but not by excision. Besides the potential for irregularities in a more visible non-hair bearing area, the incision needed for access would be in a less favorable area. The treatment is surgical electrocautery through a very small incision. This is perfectly safe because it is done below the fascial lining of the muscle. The effectiveness of the treatment takes much longer to be seen because it relies on muscle atrophy as a response to the thermal injury of the treated area.
TEMPORAL AUGMENTATION
Standard Temporal Implants

 Temporal augmentation typically refers to the building out of a deficient or concave temporal region. (anterior temporal region). Such temporal hollowing can occur from natural development, fat loss from aging, certain autoimmune diseases, significant weight loss, or from prior neurosurgical procedures. The most common approach is that if an injectable treatment using either synthetic fillers or fat. Such injection treatments can be very effective although either short-lived or inconsistent in augmentation effect in some people. When searching for a permanent solution temporal implants are available. Through a small incision inside the temporal hairline or from behind the ear, ultrasoft temporal implants are placed under the fascia on top of the muscle to create increased fullness of the anterior non-hair bearing temporal region.
Temporal augmentation typically refers to the building out of a deficient or concave temporal region. (anterior temporal region). Such temporal hollowing can occur from natural development, fat loss from aging, certain autoimmune diseases, significant weight loss, or from prior neurosurgical procedures. The most common approach is that if an injectable treatment using either synthetic fillers or fat. Such injection treatments can be very effective although either short-lived or inconsistent in augmentation effect in some people. When searching for a permanent solution temporal implants are available. Through a small incision inside the temporal hairline or from behind the ear, ultrasoft temporal implants are placed under the fascia on top of the muscle to create increased fullness of the anterior non-hair bearing temporal region.
Custom Temporal Implants
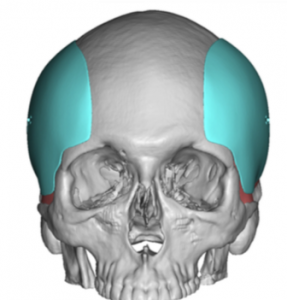 For augmentations that extended either into or are just for the posterior temporal region, a custom temporal implant design is needed. Such implant designs are intended to increase the width of the side of the head or enhance the convexity above the ears for patients who feel that their head is too narrow or pinched in appearance. These larger temporal implants are placed through incisions on the back of the ear. (postauricular sulcus)
For augmentations that extended either into or are just for the posterior temporal region, a custom temporal implant design is needed. Such implant designs are intended to increase the width of the side of the head or enhance the convexity above the ears for patients who feel that their head is too narrow or pinched in appearance. These larger temporal implants are placed through incisions on the back of the ear. (postauricular sulcus)
Temporal Artery Ligations

 One unaesthetic feature of the temporal region that is not the result of bone or muscle are prominent temporal arteries. Seen almost exclusively in men the anterior branch of the superficial temporal artery becomes visible as it courses from the temporal hairline across into the upper forehead. This serpiginous arterial course becomes most evident with exercise, heat and alcohol. It is treated with a multilevel ligation technique at various branch points to eliminate both anterograde and posterograde blood flow.
One unaesthetic feature of the temporal region that is not the result of bone or muscle are prominent temporal arteries. Seen almost exclusively in men the anterior branch of the superficial temporal artery becomes visible as it courses from the temporal hairline across into the upper forehead. This serpiginous arterial course becomes most evident with exercise, heat and alcohol. It is treated with a multilevel ligation technique at various branch points to eliminate both anterograde and posterograde blood flow.
Dr. Eppley performs a range of facial plastic and reconstructive procedures, including rhinoplasty, facelift surgery, and has helped many jawline enhancement surgery patients achieve a more attractive lower face.
Preparing for Forehead Brow Bone and Temporal Surgery
The consideration of any form of forehead and brow changes requires a thorough pre-surgical analysis. While photographs and a physical examination are usually adequate for the forehead, brow reduction may require X-rays to visualize the location of the frontal sinus and the thickness of the outer table of the bone. The forehead and brow bones can be easily viewed through computer imaging software. Every prospective forehead / brow reshaping surgery patient must be assessed with predicted computer-morphed changes. Photographs are taken before surgery and computer images are provided to the patient for review. This is an essential step in any form of facial plastic surgery requiring changes to the structure of facial bones.
Forehead Brow Bone and Temporal Contouring – The Operation
Forehead and brow reshaping procedures are always done under general anesthesia as outpatient procedures. They almost always need to be done through a scalp (coronal) incision for wide exposure and access. This will result in a scalp scar across the top of the head that ends above the ears. Endoscopic and injectable approaches are being developed, but they can only be used in a limited number of patients who are deemed good candidates. Forehead and brow bone augmentation is done by the careful placement and sculpting of various cranioplasty materials. Forehead and brow bone reductions are done by burring the outer cortex of these areas of the frontal skull. Large brow bones may require cutting off the bulging bone over the frontal sinus, reshaping it, and then putting it back into place with either resorbable sutures or very small plates and screws. For prominent or deficient lateral (tail) brow areas, the operation may be done by an incision in the upper eyelid in some cases. Forehead and brow reshaping procedures are often part of other facial structural surgeries such as rhinoplasty and jawline and chin enhancements.
Recovering from Forehead Brow Bone and Temporal Contouring
A circumferential head dressing is used after surgery to control swelling of the forehead and help the overlying tissues stick down to the implanted material and bone. The forehead will have some swelling but rarely any bruising. More substantial swelling and bruising will occur around the eyes and on the eyelids. Surprisingly, forehead surgery is associated with minimal postoperative discomfort. Numbness of the forehead and the front part of the scalp is to be expected, and it will take months for the feeling to return to normal. Sutures in the scalp are dissolvable and do not need to be removed. Forehead and brow surgery is well tolerated and infection is very rare. All patients take antibiotics for one week after surgery and take pain medication as needed.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237