Your Questions
Your Questions
Q: Dr. Eppley, I had a breast augmentation three weeks ago. I am no longer worried about any particular problems at this point as they look great. What I wonder is if the heat from a hot tub can weaken the implants in any way or cause them to prematurely break down and leach out the silicone material.? Could it weaken them in any way? I have read that it is ok to swim after they are healed but can’t find anything about what happens if they are immersed in temperatures above body level like 104 or 105 degrees. How heat resistant are these materials?
A: The answer to your question comes from the Periodic Table of Elements. Breast implants are composed primarily of silicon-based materials. Silicon is a metalloid element (#14, atomic weight 28) that is very stable and non-reactive. (it is actually less reactive than carbon) When combined with oxygen, a wide variety of polymers are created which are used to create elastomers (rubber-like materials) which make up breast implant shells and the internal gel. They are very resistant to degradation including a high heat resistance and are structurally stable from temperatures ranging from -55 degrees to 300 degrees F. Thus a hot tub poses or even a sauna that reaches air temperatures of 150 degrees F or higher poses no risk of causing any implant-related issues. This is not to mention that they are also protected by your body tissues which would suffer a burn injury far sooner than your breast implants ever would.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 25 year female and I am looking for an honest surgeon who can do a chin reduction surgery for my long chin. I am wondering if you can reduce the height of my chin vertically? I am not sure if I also need to reduce the width of my chin. I feel I have a long chin when I look at the front of my face in the mirror. To me what most important are the risks of undergoing this surgery and the outcome. I am not just concerned about nerve damage but I am also afraid of having loose/saggy skin after the chin reduction surgery. Because our skin sag when we get older, will this mean any chin reduction will make the sagging worst when we are like 45 or 56 years old…even if the soft issues was reattached and tighten properly? I look forward to hearing from you.
A: Vertical chin reduction is done by one of two approaches, an intraoral wedge reduction genioplasty and an external submental chin reduction. Which one is best for any patient depends on ow much vertical reduction they need, does width reduction need to be done as well and do they have any pre-existing soft tissue excess or sagging. In either case, the soft tissues are managed with both procedures. In the intraoral genioplasty approach the soft tissues remain attached to the inferior chin segment and and are never detached so they move up with the reattachment of the bony segments. In the submental chin reduction technique, a wedge of soft tissue is removed and tightened after the bone is reduced. In general, the submental approach is more effective at vertical chin reduction than the intraoral wedge genioplasty approach. I would need to see front and side view pictures of your chin (non-smiling) to see which approach may be best for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had chin and jaw angle implants combined with fat transfer ten days ago. I see that my lower face is much wider than expected. I realize that a lot of this is swelling and that fat transfer is overdone with the expectation that much of it will be reabsorbed. However, if there is a “window” of time that would be possible to remove the jaw implants (the chin is just fine) then I would want to be aware of that.

A: One of the very common early postoperative features of any jawline implants, including the chin, is the amount of swelling that occurs. Suffice it to say it is tremendous and doesn’t signify at all what the final outcome will be. It is actually very common that many patients in the first three weeks want to remove their implants as it just seems too big. While I am always happy to do whatever the patient wants, any judgment now is way premature and doesn’t indicate what the final results will be. As a general rule, the result of any facial implant follows the general guideline of 50% by 10 days, 75% by three weeks, 90% by six weeks and the real result (100%) by three months.
There is also the psychology of facial structural changes. Facial augmentation of natural structure is not like a facelift. In anti-aging procedures, people are psychologically comfortable with the swelling because they are just trying to go back to a place they know. (what they used to look like) Facial structural surgery is more psychologically unsettling because the person is going to a place of which they are not familiar. (a new look) This is tremendously unnerving and there is a natural tendency to want to return from when they came. If most patients can just get past this transition period (which is usually about 3 weeks, when a lot of swelling goes down) then they are usually fine and happy with their new look.
It is important to remember that the jaw angle implants are only 3mms thick, just a sliver of width really. So don’t let this temporary facial look with the swelling remotely think that the final result will look anything like what you see now. When you combine the swelling from the jaw angles with the fat grafting, it ail, temporarily look especially heavy on the lower third of the face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an occipital knob on the back of my head just like the one you have shown in your website. It’s destroying my self confidence and I would like it removed. How is it done, what is the recovery like and how much would a procedure like this cost?

A: The occipital knob is a prominent bulge of bone at the back of the head on the lower edge of the occipital bone along the nuchal line in the midline. It is an abnormal thickening of completely cortical bone that sticks out like a knob. It is most commonly a concern for men who shave their head or have very short hair. I have seen some really impressive occipital knobs that are extremely prominent. Surgical reduction/flattening of this bone knob is done through a small horizontal incision over it, usually no greater than 3 to 3.5 cms in length. (limited incision occipital reduction cranioplasty) The knob is burred down to be smooth with the surrounding bone. Usually I will then suture the soft tissues down to the bone surface through bone holes to make sure no fluid develops between the skin and the reduced bone. The skin is then closed with small dissolveable sutures. This procedure takes about one hour under general anesthesia and is done as an outpatient procedure. The cost of the procedure, all expenses included, can be obtained by contacting my office for a quote.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am seeking gynecomastia reduction. I have hard lumps bilaterally under each areola. I am a 32 year old male and would like to have them surgically removed. I have a toned muscular body and It is somewhat annoying. I’ve had this condition since puberty and it hasn’t resolved. They are visible through shirts and when I’m shirtless or in the water it is somewhat noticeable. What is involved in getting this condition resolved?
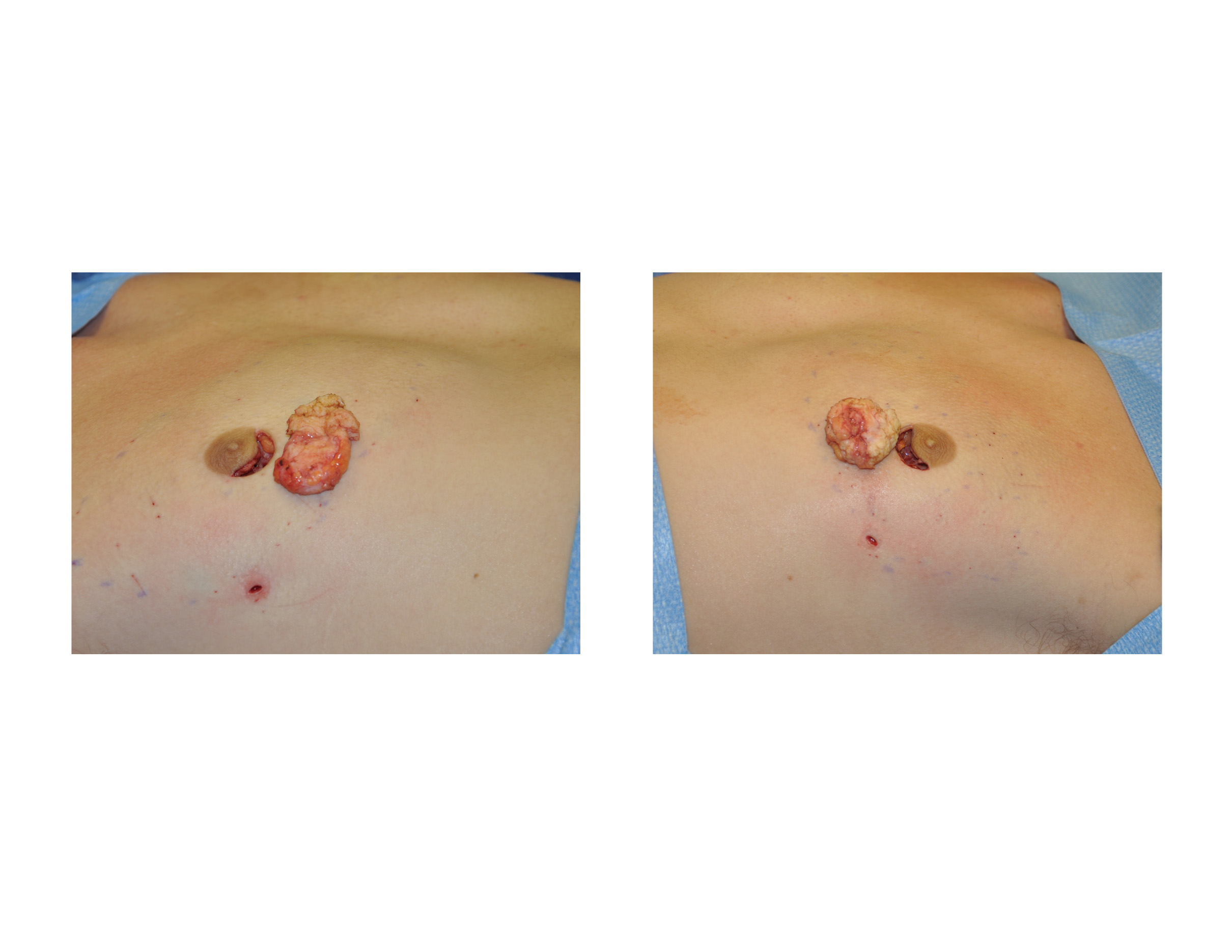
A: It certainly sounds like you have areolar gynecomastia which appear as isolated hard lumps under the nipple. There may also be extra breast tissue that is softer that extends outward from these hard lump areas. This type of gynecomastia reduction is done through inferior areolar incisions including the liposuction portion if needed. Most such areolar incisions heal imperceptibly. This is done as an outpatient procedure under general anesthesia. Drains are not usually used for such limited male breast tissue excision procedures. Recovery will take a few weeks until you can return to full activities including strenuous exercise.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, when you do liposuction do you close the incisions with stitches or staples or just leave them open? A relative of mine across the country had liposuction recently on her stomach and thighs and they didn’t close her incisions. I didn’t realize that liposuction was done that way. She said her incisions bled for days and she had to keep changing her wet bloody garments. How does this affect the liposuction result and does it increase the risk of infection?

A: Whether a plastic surgeon chooses to close liposuction incisions is a matter of personal preference. There is no evidence that not closing these incisions increase the risk of infection or affect the outcome of the procedure in any way. It is common for the liposuction incisions to leak fluid for 24 to 36 hours after the procedure which is primarily induced by the wearing of the compression garments. (squeezing it out) What one sees, although it looks like a lot of blood to the patient, is actually just a little bit of blood mixed with the tumescent solution that was infused at the time of the surgery. One could argue that the more this fluid comes out the less swelling and bruising that will subsequently occur. If the fluid does not come out it stays in the body and must be absorbed over time as one heals. If the incisions are closed probably less fluid comes out but a fair amount will still ooze out anyway. This is why I tell patients to not sit or lay on anything they value (without a blanket) for the first few days after surgery.
That being said, I do prefer to close my liposuction incisions (with the exception of those placed inside the belly button) as it increases the likelihood of better scars, small as they may be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, years ago I had a brow-bone reduction surgery for facial feminization. Unfortunately, the surgeon I chose tried some novel procedure that ended up leaving me with a missing anterior sinus wall and bone chips lodged in my frontal sinus. Another surgeon, an ENT, then obliterated my frontal sinus with hydroxyapatite. This fixed the air leaks and replaced the missing bone, but left obvious irregularities in my forehead. I recently had a CT scan done and discovered that he also failed to completely obliterate the sinus; there is still a cavity on the left side. I came across your page while doing research and discovered that you had a lot of experience in forehead work as well as craniofacial experience, and I was wondering if this was something you think you could fix. I’m hoping to have the last of the sinus obliterated with hydroxyapatite or similar and to have the defects in my frontal bone filled.
A: In doing brow bone reduction surgery, removing the anterior table of the frontal sinus and putting it back as morselized bone chips is not going to be a successful strategy. (as you have discovered) This will leave one with significant indentations and irregularities over the brow bones. Repairing this problem with frontal sinus obliteration by mucosal lining removal, obliterating the frontal sinus ducts with bone grafts and then filling it with hydroxyapatite cement up to the level of the desired brow bone shape is the correct treatment. However if one fails to get out all the lining or does not obliterate the frontonasal ducts, a residual frontal sinus cavity will remains which could be a source of infection.
I am going to assume that this residual sinus cavity is located near the frontonasal ducts underneath the hydroxyapatite cement. If this asymptomatic and the cavity is clear, then I would just fill in the outer brow bone contour and leave it alone. However, if it is a source of pain or frontal sinus infections, then it should be removed and obliterated with cement along with the brow bone/forehead contouring.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in deltoid implants which amongst other procedures as I learned you are very skilled at. I have pictures for my shoulder which are attached. The dimensions for the augmentation are 16cm measured from clavicule down lateral view to end of the deltoid in the center line, the widest part is around 10cms with a projection of 2 cm.

A: Thank you for sending your shoulder augmentation desire and dimensions. Deltoid implants are one of the most uncommon type of body implants but requested for them are becoming more frequent. One of the reasons I asked for them is to have a vision as to where the patient sees the location of the deltoid augmentation and the dimensions that the implants have to be. As there is no off-the-shelf premade deltoid implants, I have to either use an existing style of body implant (usually a calf implant or a custom silicone carving block) or have a custom one made. As it turns out there is an existing silicone carving block with the dimensions of 16 cms long, 9 cms. wide and 2 cms. high. So that does fit the dimensions you have given although although that is probably a bit big. A more appropriate deltoid implant size would be 14cm long, 7 cm wide and 1.5 cm high. The other consideration is knowing the location and the implant size I have think about the incisional location to put it in during surgery. Usually this is done from the back side of the shoulder rather than a direct incision over it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a 38DD and my breasts sag slightly. I have been treated for back pain for several years. My question is…is it difficult to get this procedure covered by insurance? I’m very interested in getting a breast lift but could not pay the entire bill out of pocket. Should I even try to pursue this?

A: To answer your question, the first thing to determine is whether you are trying to achieve a breast lift (with no reduction) or trying to get an actual breast reduction done. (smaller breasts with the lift that comes with them) Breast lifts are never going to be covered by insurance as that is a cosmetic procedure. Conversely many breast reductions are covered by insurance as they improve back, shoulder and neck pain as the size of the breasts are reduced. Thus they are often viewed as medically necessary and may be covered. But their potential coverage has to be determined before surgery by a predetermination letter which documents your breast size, the symptoms associated with them and how much breast tissue will be surgically removed. From this information, the insurance company bases their decision for coverage.
But when it comes to breast lifts, there is no purpose in trying to see if insurance will pay for it as that can be determined right now…there is no medical need and thus no insurance coverage for the operation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I’m 23 years old, and I would like to have breast augmentation. But I am a petite person and a ballerina. I wouldn’t want anything bigger than a medium B cup, is that possible? I really don’t know the difference between the types of breast implants so I don’t know which is best for me. How much does this surgery cost? Thanks.
A: Any size breast augmentation can be done, even for very small size requests. Implants comes in volume as small as 100ccs and go all the way up to 800cc in silicone and 960cc in saline (can be filled that volume from a 800cc implant) The cost of the surgery is somewhat dependent on the type of breast implant used so knowing what you would want is important.
While both saline and silicone breast implants are available, FDA-approved and can create excellent breast augmentation results, there are some differences between them that every woman needs to fully appreciate. While saline breast implants costs less (total cost $3,999) and can be placed through the smallest incision, they will one day suffer catastrophic failure (deflation) and are prone to developing rippling on the bottom edges of the implant in women who are thin with little breast tissue. Silicone implants cost more (total cost $4,999) and require a slightly larger incision to put them, but have virtually no rippling (most natural feel) and do not fail by deflation but by a ‘silent rupture’ process in which the breast does not lose volume or size. Because of the delayed awareness of an implant problem (which is harmless) silicone breast implants will last longer.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am in need of jaw angle implant revision surgery, I had large, off the shelf, silicone jaw implants done two weeks ago. To me (at this stage) they look too big and are asymmetrical. As you can see from the photographs there is a distinct difference to both sides of my face, with one jaw side being lower than the other. i am also concerned that they bulge and “round out” my face from under the ears. also believe they made my face longer and squarer. I want badly to correct this and if this entails customized implants that achieve (or approach) symmetry, I hope you can help.

A: Let me start by first making a general comment about jaw angle implant surgery in men. Just about every patient in the first few weeks or month after surgery thinks that the implants are too big, asymmetrical or both. While they may very well be (I obviously don’t know what you looked like before and what your aesthetic goals were…and the beard adds another visual element which may or may not be helpful in interpretation of the results), what is important to know is that 50% of the final result is seen at 3 weeks, 75% of the result is seen by 6 weeks and it takes a full 3 months to see every detail of the final result in any form of facial skeletal augmentation surgery. So at just two weeks after surgery what you are currently seeing may or may not be a harbinger of the eventual outcome of the procedure.
I say this because I have seen numerous men jump too quickly into jaw angle implant revision surgery…long before the final result was apparent. There is an accomodation phase to the new look and that does not happen for most patients in the swelling phase of the recovery period.
The two most common complications from any facial implant surgery, in particular jaw angle implants, is what you are feeling now…over/undersizing and asymmetry. Given that you are still somewhat swollen it it hard for me to know what look you were trying to achieve and what makes the way it looks now not desired. Did you have computer imaging done before our surgery to get a feel for the look you could achieve in your face? Your description suggests that they are too big (wide) and are of a lateral design…which would account for the rounded lower face look. I suspect these are 11mm wide lateral angle implants. Such dimensions can also make the face look more square and longer (which is what many jaw angle patients want) but this style implant has very rounded edging.
Jaw angle implant asymmetry is a function of placement and how secure the implants are onto the bone. They were placed from inside the mouth but where they secured with screws?
I ask these questions because the solution to your jaw angle implant concerns may already lie within you (modification of existing implants and their positioning) While custom implants can always be made, I would first look at whether what you have can be salvaged to the right amount of jaw angle augmentation and symmetry…consisting of the simplest and most economic approach to jaw angle implant revision surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need earlobe reconstruction. I’ve stretched my earlobes to two and a quarter inches. I’ve decided I want to get them fixed and I know you are the surgeon who is best at this. I was wondering how long will I need to let my earlobes shrink before getting the surgery?

A: I would allow them to shrink down for a minimum of 6 weeks, which will be about 75% to 90% percent of how much they will shrink. Usually three months is tehe time when 100% shrinkage has occurred. That is sort of a standard protocol since there is rarely is a need to fix them on an immediate basis. But having done several urgent cases where the earlobes have torn from overstretching and having fixed both sides at the same time, the outcome has been the same whether the earlobes were allowed to shrink down or not. This is not surprising since what is really expanded is the outer rim of earlobe skin which gets removed anyway. It is just smaller if the gauges are removed beforehand. The adjacent earlobe tissue around the gauged site (whcih is what is kept to reconstruct the earlobe) does not change that much.Thus I do not believe it matters greatly whether you allow the earlobes to maximally shrink or not. But if you have the time then I would do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a fat injection breast augmentation done one month ago. I took a vacation one week after surgery and I was fine. Well exactly two weeks after my procedure I noticed my left breast was bigger, swollen, tender, painful, and very warm. I thought nothing of it and my doctor said it was normal. When I questioned why my right breast didn’t feel that way he said each breast healed differently. Well the next day after my symptoms got worse and I felt dizzy and weak. I woke up soaked and noticed a yellowish pinkish discharge leaking from my left breasts incision. I ran to the ER and was admitted for 6 days. I had an abcess and required surgery for drainage. I was given a lot of antibiotics and I’m now having to clean and change dressing twice daily. This has been a total nightmare! How long will it take for my infection to go away and for pus to stop leaking? When will my incision close if I have no stitches? I’m afraid my breasts will now look deformed and different in size but im terrified to get another procedure done for correction. What caused my infection? Why only my left breast? Could too much sun exposure, drinking, and pool have caused my infection?

A: Sorry to hear of your very unfortunate complication. While using your own fat for breast augmentation is a natural material, that does not exclude it from the risk of infection. (although that risk is probably lower than with implants) Because the injected fat has no blood supply and must acquire it after being transplanted, there is a period of time after surgery when infection can develop. That is usually between 10 and 21 days after surgery, the time when you are off antibiotics and bacteria have had time to multiply and grow.
Almost all infections that occur close to surgery, regardless of the procedure, occur because some bacteria go into the wound during surgery. Why it occurred in one breast and not the other will never be known but fortunately it was just one breast.
Once you have developed an infection around injected fat, there will be fat loss or less take in that breast. Probably what you have coming out of your wound now is mostly liquified fat rather than pus which is injected fat that is breaking down due to the infection.It will probably two to three weeks until this clears up and heals.
That breast should be allowed to heal for a year, get soft to the feel, and see what the final amount of fat take will be. I suspect there will be some breast asymmetry due to different amounts of fat take per breast. Correction of that breast asymmetry, if it occurs, will be by additional fat injections. Just because you have had this complication does not expose you a subsequent or higher risk if you have the procedure done again.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in some type of forehead reduction. I am a young woman and I’m not happy about my face at all. The biggest problems I have are with my jawline and my frontal bone. I also have really deep insetted eyes. I’m kinda chubby but I used to be skinny and I had to exact same problem. I have big cheeks , something like squirrel cheeks and jowls on the side of my face. I really want a nice tight jawline. When I tighten the skin together and pull it through my ears I see it the way I would want it to be. I was wondering if that is possible for me without having a jawline surgery.
I have a very big frontal bone and I would love to have a nice flat forehead like most women have. I was wondering if that is possible for me to get it flattened. Maybe there is also someting you could do for my deep insetted eyes. I want to send you some picture’s and I’m wondering if you could look at them yourself and if you have any tips for me to make me as beautiful as possible.
A: Thank you for your inquiry and sending your pictures. The most effective procedure that you could do for your face would be a combined orbital/forehead reduction and hairline scalp advancement. This would reduce the depth of your eyes, lessen the brow ridge prominence, and make the forehead look smaller.
Only a jowl lift can create the desired look you are after along the jawline and you are too young for that procedure. There are no non-surgical methods that can create the same effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in scar revision surgery. I have a transverse abdominal scar from surgery I had as an infant. It is “socked in” . My skin is adhered to my muscle and there is an overhanging lip above the scar. I am 27 years old. I also have a vertical 4.5 inch scar below the belly button I would like to have lightened. It is two years old.
A: It is very common to see scars from abdominal surgery done as an infant to be completely adhered to the muscles. This is because at such a young age there is little to no subcutaneous fat between the skin and the muscle. The incision line scars down to the muscle (as there is little to no fat interface) and appears as an indented fixed line as fat tissue develops between the skin and muscle around it as the patient gets older. This can be dramatically improved by scar revision surgery by cutting out the scar, releasing the surrounding tissues from the muscle and advancing and closing the skin edges together. While a scar line will still be present, it will be leveled and a much narrower scar. Such scar revisions can often make for a dramatic change in the appearance of such scars.
When it comes to scar lightening that is a different matter. There are not many effective therapies for scar discolorations other than to cut (excise) out the scar.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have two issues: 1) a birthmark the full length of my cheek which I’ve had my whole life and 2) the facial hair covering the birthmark is substantially thicker than that covering my other cheek. Can you help with either of my two issues? Photos attached.
A: What you have is a congenital nevus of the face. Its characteristics are well known and include being born with it, the involved skin is thicker and more pigmented and the hair that grows from it is often darker and thicker. The key concept to understand about congenital nevi is that involve the full thickness of the skin. Thus they can not be removed or reduced by laser resurfacing or treatment method. The entire full-thickness of the skin needs to be cut out (excised) either through serial reductions or as a single surgery and then covered with a skin graft. While this would cure the nevus, it would result in a worsening of the aesthetic appearance of the face and I do not believe you would consider it an improvement. This is a long way to say you are better off to leave it alone as the treatment of it is worse than the problem.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have breast asymmetry and am interested in breast augmentation/lift surgery. I am 18 years old and have had two children. My breasts are significantly different by at least two cup sizes and have been so for six years. I have Tricare insurance. I am wondering if my being 18 years old is ok for breast surgery because I have already had two children so my body is done growing. I’ve spoken with my family doctor about wanting to have this done because its already done a lot of physiological damage to me.
A: Significant breast asymmetry is always a challenge in any form of cosmetic or reconstructive breast surgery. Having had two children and being two cup sizes different almost certainly speaks to the potential of needing some form of a breast lift on at least one the breasts (usually the larger one) and perhaps implants for both. Until I can see some pictures of your breasts I can not be any more helpful in recommending a specific plastic surgery treatment plan as there is great variability in many cases of breast asymmetry.
What is known now, however, is that insurance is not going to cover this type of breast surgery. Unless it is a case of reconstruction after breast cancer, breast reshaping surgery will be considered as a cosmetic procedure by any insurance provider today. The fact that you may have developed this through no fault of your own and it has a significant negative impact on your self-esteem is something that I have learned carries little weight with insurance companies.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for extreme jaw angle augmentation. I recently came across a paper that described a technique for mandibular angle augmentation, where segmental distraction osteogenesis and rib cartilage transplants were used to achieve the desired effect. What I found notable was that the degree of vertical augmentation and the extent to which the jaw became “square” was extreme, beyond what I have traditionally seen achieved with implants. For reference, I have included the before/after pictures from the paper below.
My questions are:
1. Do you (or would you) ever perform distraction osteogenesis to vertically lengthen the jaw, without affecting the bite?
2. Assuming you do not perform this type of surgery, would custom implants be able to achieve the same effect to the same degree?

A: That is an extreme approach to jaw angle implant augmentation for which there is a much simpler technique to get to the same place, custom jaw angle implants. I have done numerous jaw angle implants that drop the angles down as much a 25 to 30mms. I see no reason to ever do a distraction technique to achieve that kind of jaw angle result. What that paper is not showing you is the long-term result of that technique of which I will wager that much of the jaw angle lengthening either relapses or resorbs….not to mention the notching that undoubtable develops between the anterior edge of the distracted bone segment to the normal mandible in front of it. The x-ray shown does not show bony consolidation across the distraction site…probably because it does not occur in an adult. Such a result demonstrates that it can be technically done but that does not always mean it is a good thing to do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in facelift surgery. I am 55 yrs old and have been single for twenty years. I want to finally get to the place were I feel wonderful about me. I do not want to look like a different person with a drastic change. Is it really possible to have the face procedures to look younger/fresher and still be me? Seriously, I hate what I see on TV from even Hollywood stars who have all the financial resources I could not even imagine.
A: Despite what you see from Hollywood celebrities, that is not the way the vast majority of facelift procedures turnout. Unlimited financial resources do not necessarily allow one to make better choices, often the reverse is true. Being able to do anything doesn’t always mean you should. It is also important to understand that those who are in the spotlight on a continual basis face a whole different set of pressures from an appearance standpoint than you and I do. Lastly the face and body standards in Beverly Hills and Hollywood where most of what you see comes from is much different than here in the Midwest. Just walk around those areas and you will see what I mean.
The reality about facelifts and other facial rejuvenation procedures is the opposite of what you think. It is almost never an issue of ‘doing too much’ but can enough results be achieved to make the patient happy. When it comes to facelift procedures, no one ends up looking like a different person. The key is to do the right combination of facial rejuvenation procedures in a judicious manner that makes one look better and younger and not ‘overdone’.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in brow bone reduction surgery. In the past few months my brows have started to be protrude. Is there anything that I can do to stop it or how much would it cost to have it remove or is their payment options? Its really affecting my way of life.
A: Brow bone reduction surgery is always an option for brow ridges that have excessively overgrown. Your brow protrusion, as long as it is symmetric (and it appears so in your pictures) is the result of a pneumatization process. (development and expansion of an underlying air cavity) While not present at birth, the frontal sinuses have a fair degree of development by 7 or 8 years of age but continue to grow (expand) until well after puberty. Why some people develop bigger frontal sinuses than others is not clear other than due to hormonal influences. (men develop bigger frontal sinuses than women hence the development of the stronger male brow ridge) Spontaneous frontal sinus growth after puberty could be the result of a late pubertal spurt, medications such as steroids or a more conscious awareness of its size.
While brow bone reduction surgery can be done (usually an osteoplastic flap setback is the most effective technique), this requires a scalp or coronal incision way back in the hairline. While this can certainly be done, men always have to think very carefully about this scar trade-off. Given that you shave your head this consideration is of high significance. Initially this is a far more important hurdle to cross than that of the cost of surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in fat injection breast augmentation. I have a consultation coming up with you next week and was wondering if you use the Brava before fat transfer for breast expansion? I was wanting to get into surgery ASAP as I am going on vacation next month and want the surgery prior to the trip. If I have to wear the Brava, I won’t be able to get the surgery done before the trip and be healed enough to wear a bathing suit. Also, I would prefer conscious sedation to a general if you do that.
A: If your goal is to have a completed fat injection breast augmentation within the next thirty days, that is not an achievable goal. Breast augmentation by fat injections, if you are a good candidate (and most people aren’t) requires 3 to 4 weeks of presurgical breast stimulation by the Brava device followed by a similar time period after surgery of use of the device. This is an optimal device, even though it is inconvenient, as it provides stimulation to the breast tissue and the injected fat so that its survival is optimized. Thus you can quickly see that is not going to work by your desired schedule. The only way that time period works to enjoy the benefits of breast augmentation by your vacation is the placement of breast implants. In either case, however, both are best done under general anesthesia. Successful breast augmentation, by any method, is not something to be done under local or sedation anesthesia without suffering a suboptimal result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a few questions regarding the chin and jaw angle implant procedure. I know you are very busy as a surgeon but if you had a few minutes of free time, I would appreciate it if you could answer some questions before our consultation. It would probably save time for both of us as well. Regarding the Mandible Jaw Implants, I’ve been researching online that this procedure is riskier than chin implants and that they tend to have a higher rejection rate. I’ve also read that they require a very skilled surgeon who has a lot of experience with this procedure. I’m sure you can understand my concerns, so here are my questions:
1) How many mandible/jaw implants (NOT just chin implants) have you done in the past?
2) How often does infection occur with jaw implants and how often do patients request to have them removed (either from infection or dissatisfaction)?
3) I’m looking for that “Chiseled Look”, or angular looking jawline which you see on many famous actors or male models – not necessarily a massive or fat looking jaw – but a defined/contoured jawline. Assuming one has a low body fat percentage, is this look possible with a jaw and chin implant? Also, will the jaw/chin implants look natural in that they look contoured to the face rather than just a large mass hanging from your lower face?
4) How long does recovery take for both a Chin and Mandible Jaw Implant procedure? I’m starting a new job soon so I’m probably going to give myself 2 weeks in between leaving from my current position and the start date for the new job. Would 2 weeks be enough time? It wouldn’t make the best first impression to walk into my new job on the first day and have a swollen jaw, haha.
5) Are the Mandible Jaw Implants customized for different size faces or are they “One-Size-Fits-All” ? I noticed some doctors use customized ones and some use standard implants. Is there a major difference in looks between the two types?
6) Finally, I noticed there are not a lot of Before and After pictures of jaw implants on the internet. Is this because the results don’t turn out good or it because its just not a common procedure? Would it be possible to see some of your jaw implant work during our consultation?
A: In answer to your questions:
- I have performed over 100 standard or custom jaw angle and jawline implants. (and many more chin implants) You are correct in that it is a harder facial implant procedure to do and is not a mainstream facial implant procedure done by a large number of surgeons.
- The infection risk with jaw angle implants is not higher than any other facial implant although the material of which they are made can affect that risk. (Medpor has higehr risk than silicone) Expect a 10% to 15% risk of revision which is usually for asymmetry or unhappiness with the size. (too big or too small)
- The only male patients that can achieve a ‘chiseled’ look or a male model look are those men that have a lean face where changes in the skeletal contours are most easily seen. With today’s implant shapes and designs there is no such result as the implant looking like it is ‘hanging from the bone’.
- Two weeks is really not enough time to recover from a facial appearance standpoint. Three weeks is more realistic.
- Both standard off-the-shelf implants as well as the option to customize them are available. Which approach a patient takes depends on their aesthetic needs and their budget.
- Since few plastic surgeons do this kind of facial work, it is hard to find many examples of results. My work is fully reviewable on my website at http://eppleyplasticsurgery.com//jaw/ under the patient photo section.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to know about facial fat injections. I know a 24 year old who is unsatisfied with her facial appearance. She weighs 118 lbs, and is 5’6”. She does have a lot of facial fat especially in her lower cheek and the areas around the mouth. Ironically, this makes her mouth look fat. She has had braces, but is still unsatisfied because she says that the most noticeable part of her face is still her mouth. She is pretty, but she does not smile because the “excess skin makes creases” at the sides of her mouth. I did a little research and deduced that she has noticeable perioral mounds due to a lack in facial volume. Do you offer fillers such as sculptra and radiesse, or would fat transfers to the cheeks be possible and could this possibly improve her appearance to a noticeable extent? She is doing all she can to avoid getting cheek implants. She is so young to be unhappy about her face.
A: Some of what you ate saying is a it contradictory. Perioral mounds are excessive collection of fat just to the sides of the mouth. They do not occur ‘due to a lack of volume’ as you have described. You may have mispoken in that regard. Thus I am not sure your friend had too much fullness at the perioral mounds or a lack of it.
Injectable fillers are always a good first step to try if one is uncertain whether the addition of volume is the correct facial approach. If one is certain that the addition of volume is needed, facial fat injections would be a better approach as it has the potential to offer some permanency while synthetic fillers do not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can I benefit from cheek implants? I have a long thin face that has always bothered me. I don’t know what if anything can be done to add fullness or reduce length? I always look like I am scowling and as I age…it gets worse. The first picture attached us awful I know but it at least gives you an idea of my situation. The second pic is simply one I have played with to widen my features and wish were possible. Thanks for your time.
A: There are improvements that can be made to a long thin face in terms of both length and width. Facial height reduction options are more limited than those of width and are often relegated to the considerations of vertical chin reduction, upper lip lift (shortening) and in some cases rhinoplasty. Numerous facial width increase options include jawline and jaw angle widening, cheek implants and fat injections between these two skeletal area. (the trampoline facial zone) Which one(s) of these might be most beneficial to your face depends on a computer imaging analysis. Unfortunately your one picture is not adequate to much of anything with due to the poor picture quality. If you could send me a front, quarter and profile views of your face (non-smiling) I would be happy to do that assessment for you. Based on this one picture it does seem that cheek implants may be helpful for more facial width and that could be combined with fat injections for a more blended transition from the implants into the thinner and non-bony supported areas outside of the cheek zone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to have a chin dimple made to look like Adele’s chin. Can you do that and how is it done?

A: What you are asking about is chin cleft creation surgery not the creation of a chin dimple. In looking at the chin of the singer Adele, careful assessment will show that what she actually has is a chin cleft and not a chin dimple. This chin feature distinction is not really semantics but two distinct anatomic entities. A true chin dimple appears on the center of the chin pad above the lower border of the bone and is a circular indentation. It occurs as a result of an underlying soft tissue (fat) deficiency without a mentalis muscle defect. Conversely a chin cleft appears on the lower end of the chin pad and is a vertical groove that crosses the lower border. It can have a wide range of depths from just a very shallow hint of a line to a very deep groove. Chin clefts are the result of an actual mentalis muscle defect (midline separation) and may actually involve a groove in the underlying chin bone as well.
In the surgical creation of chin dimples and clefts, this distinction is critical as the technique to do them is different. As a general rule, successful creation of a chin cleft is more reliably done than that of a chin dimple. Chin cleft surgery is best done from a small incision on the underside of the chin, a groove is made in the bone, a strip of soft tissue including muscle is removed above it and the underside of the skin sewn down to the groove made in the bone. It can also be done intraorally but it is technically more difficult and I have found it to be not quote as reliable in terms of getting a good result. This is a small outpatient procedure that can be done under local anesthesia or IV sedation. Other than some mild chin swelling there is no real recovery afterwards. Expect that to see the full depth of the chin cleft result to take about six weeks.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an intraoral large silicone chin implant placed about nine years ago and have had a lot of chin implant complications. am 31 years old now and since the beginning I got into a cycle of pain from chin swelling followed by tightness, numbness and itching sensations. Rare were the moments where my chin wasn´t swollen and pain free. The itching is basically in my right cheek. Four years ago I had a fibrosis inside this right part of my face and the doctor thought it was due to the tip of the implant so he had cut the cheek from the outside and cut the tip of the implant filling the hole left from the fibrosis with body fat. The appearance from the right cheek didn´t improve much and from then on I had to carry a scar from the procedure. About a year ago I had a fistula in the right gum that bleeds weekly. I´m terrified about the implant removal procedure been performed by the same doctor, the pain not going away due to eventual permanent nerve damage and bad looking chin appearance after removal. Do you know how to solve this by eliminating the pain and also leaving me with a good looking chin?
A: Chin implant complications of this magnitude are rare. I am not sure why you have such symptoms of itching and chronic pain but this long sequence of events suggests that the implant should be removed and your chin augmentation done with a sliding genioplasty. Moving the chin bone would eliminate any potential concerns about a foreign body in your chin and all the issues that have accompanied it. I would need to see some pictures of your chin for your further assessment but this does not sound like an implant salvageable situation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, is there a mouth widening surgery? can a mouth actually be enlarged? My mouth is so small dentists literally have difficulty working inside. One told me it was the smallest mouth he’s ever encountered (I’m not making this up). A 1/4 inch more would make me and my dentist infinitely grateful. But is that possible?
A: Yes a mouth can really be enlarged or made wider (longer) from a horizontal standpoint. Known as a lateral commisuroplasty, the corners of the mouth are opened up and the horizontal width (length) of the corners are expanded. This is done by making a 1/4 inch (6mms) incision in the skin from the vermilion-cutaneous junction horizontally outward. Then the vermilion lining (pink part of the lip) is advanced from the inside out to make a new lining and corner point. While an incision is necessary, all scars line remain along the vermilion-cutaneous junction (skin-lining edge) and not beyond the corners of the mouth. When done on both sides this amounts to a 1/2 inch mouth widening. When you factor in scar contracture of about 25% to 33%, that still leaves one with a 1/4 inch or more increased mouth width.This is a very simple procedure that can be done under local anesthesia.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I found a comment from you on the internet regarding burn scar revision. The reply seemed very honest regarding how to treat burn scars….meaning it is very difficult to treat and a 100 % elimination of it is not possible. My daughter is 14 years old and when she was 4 she was involved in a terrible accident, which left her with a 3rd degree burn scar on her forehead. Now the teenage years has begun and that is very difficult for her, as the focus from other teenagers constantly is her scar. We have tried laser surgery with limited success. The main challenge is the dark colour surrounded by a white scar colour and then the normal skin. What kind of solutions do you see, if any. Please let me know or perhaps I can sent you some photos. Thanks a million in advance for your reply from a very desperate father.
A: While I would need to see some pictures of the forehead scar to give a more definitive answer for your daughter’s case, I can make some general statements about burn scar revision. Burn scars are the most difficult of all scars to treat because they are broad-based and the involved skin, and sometimes the surrounding skin, is not normal. Pigment has been lost and the healed burned skin is not normal. There is just no way to ever make burned scar acquire pigment (the melanocytes in the skin layer has been lost) or achieve normal elasticity. Some texture changes in the skin may be possible by fractional laser resurfacing but you can not stimulate abnormal skin to become normal skin. The surrounding hyperpigmentation of the unburned skin can also be very difficult to eradicate. While some mild improvements may be possible with fractional laser resurfacing and pulsed light treatments, significant changes are not usually seen and the results will always be less than what any patient desires. In some cases, the burn scar is more linear and it may be able to be excised back to normal skin. There will always be a scar but this type of burn scar revision makes for more significant improvement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know if you actually do silicone drop down jaw angle implants. Where I am from not many people do it here. I am not a big fan of Medpor. Roughly how much would you charge for this procedure as I am saving up. Let’s say if you do have a drop down silicone implant can one get a few mm width as well? Iwould like a bit of a square look from front but not too extreme as I have a skinny skeletonized face? On the picture I have uploaded my right side jaw as without the beard I do not like the shape of it. I would like the jaw angle to go back towards my ear and possibly a small drop down so my face does not look too long. Personally I think my chin is fine and my jaw isn’t too bad as some peoples but I’d like it to be more square from the front and from the side. I have also took a picture of my front face and as you can see it is a bit more chiseled. I am hoping I can achieve this look like in my after picture since my face is skinny. I’d preferably like silicone.
A: The concept of vertical lengthening jaw angle implants made of silicone is one of which I am quite familiar. Historically silicone jaw angle implants could only add width and not vertical length, a flaw in their basic design. Snce most patients that want jaw angle augmentation have a high jaw angle position, vertical lengthening is one of their most important dimenions. I am working with a major silicone facial implant manufacturer on these new jaw angle implant designs which will have various length and width dimensions to them. With a silicone material these implants will be easier to insert as well as revise/remove should that be necessary.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very sorry to disturb you, I live in a remote area of Russia, and my grandson was born with craniofacial distortions of his face and skull. My friend found your contact details in the Internet. I have a few questions to you:
1) Is it possible to enhance at the same time (by one surgery) my grandson’s forehead and back of his head? They are both too flat and the maximum distance between his eyebrow line and the back of the head is 14.7 cm only. By how much is it possible to make this length longer?
2) What should it be done with his medium face? Will it be the treatment by implants, or it is possible to put there human grease/fat?
3) What else could you recommend on him ? We know that he also needs the surgeries on his jaws.
4) How much will it cost us to get the above mentioned treatments ( 1) and 2) points) at your clinic in the USA?
Thank you so much for your reply.
A: Thank you for your inquiry. In looking at your grandson’s pictures, it is clear that he was born with some form of craniofacial deformity, most likely one of the craniosynostoses. (Crouzon’s etc) It also appears based on the scars on his forehead that he may have had some initial efforts at craniofacial surgery when he was younger.
While you did not state his age, he appears to be a mid-teenager at least. I will separate his craniofacial concerns for this discussion into cranial (skull/forehead) and face.
From a skull standpoint he has a short front to back distance typical of many congenital craniosynostoses. He is shorter in the back than in the front in my assessment. The back (occiput) can be augmented significantly (up to 2 cms.) and the forehead smoothed out for a better contour. The most relevant issue here is where is his previous coronal (scalp) incision as that will determine how to approach is skull augmentation reshaping.
From a face standpoint there are two directions to go. Ideally he needs pre- and postsurgical orthodontics and a LeFort I midface advancement with a sliding chin genioplasty. The key there is orthodontic preparation. If this is not possible, the second approach is to camouflage the bony deformities by a combination of orbital, cheek and paranasal implants combined with a sliding genioplasty. (see attached imaging) That could be done at the same time as skull augmentation.
The key in any complex craniofacial problem in a mid- to late adolescent is to identify those craniofacial surgery procedures that are most practical to do that provide the greatest physical and psychological change for the patient.
Dr. Barry Eppley
Indianapolis, Indiana