Your Questions
Your Questions
Q: Dr. Eppley, I am interested in chin augmentation. I am a 52 year old male in good health with no serious medical conditions. Three years ago I had a platysmaplasty, rhinoplasty, lip lift, and implants in my chin, jaw angles, and cheeks. The chin implant subsequently became infected. The infection resulted in the removal of the chin and jaw angle implants several months later. Only the chin implants remain. My primary concern now is that my chin appears weak. I’m also concerned about the sagging appearance on underneath left side of my chin and the very visible scar below my chin from the previous surgeries. Regarding the jaw angle implants, I understand that my posterior mandible is quite narrow, but my eyes are also narrowly set and jaw angle implants accentuate that feature. I learned this clearly from the very wide jaw angle implants I had from my first surgery. So, jaw angle implants are problematic for me for that reason. Also, the chin and jaw angle implants that I had moved significantly after surgery, which I would also like to avoid with any subsequent implants. Please let me know if you can fix any implants with screws so that they do not move.
A: In reading your history, you have lost the benefits of your chin augmentation due to infection, your implants shifted after surgery and the jaw angle implants were an aesthetic detriment. In addition the submental scar is very wide and there is a little tissue sag on the left side of the chin.
A new chin implant can certainly be done and I almost always secure this in by double screw fixation. This could be put in from your existing submental scar. Your submental scar is wide because it has been placed behind the submental skin crease in the skin of the neck. This is not an ideal location as horizontal incisions in the neck skin tend to widen. The best that can be done with that scar is to excise it completely and hope that it heals more narrow this time. A new chin implant should pick up any loose skin along the jawline.
Jaw angle implants are more than just about widening the jaw angle as you appear to have had lateral widening jaw angle implants used. There are also different styles of jaw angle implants that merely make a pronounced jaw angle without making it wider. You may initially have just had a wrong style implant used.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking for a rhinoplasty that can get my nostril size reduced. I would like to reduce how much of my nostrils you can see from a front profile ( basically bring the front of my nose down). Lastly I don’t like how you can see in my nostrils from the side profile. Does this all seem possible?
A: From a rhinoplasty standpoint, the size of one’s nostril’s is controlled by several anatomic factors. These include the length of the lower alar cartilages, the amount of caudal septal support, the angulation of the lower alar cartilages away from the dome and the width of the nostril base. When looking at your nose, the main reason you have a lot of nostril show is that the length of your nose is short making the tip of your nose rotated upwards. (which is why there is excessive nostril show in the front view) In addition, you have alar rim retraction with a bowed rather than straight alar edge. (which is why these is too much nostril show in the side view)
To increase your nasal length and decrease nostril show, your rhinoplasty must have increased structural support. This is done through cartilage grafts, harvested from the septum or ears, placed to push the tip of the nose down (septal extension graft) as well as along the edge of the lower alar cartilages. (alar rim grafts) You may also benefit from nostril narrowing as well but that can only be determined by a front view picture which you did not provide. I have attached some imaging to show what this type of rhinoplasty can do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Is wisdom teeth removal a prerequisite for an osseous sliding genioplasty? Also, how much does your practice charge for an osseous genioplasty (with hospital fees + anesthesia)?
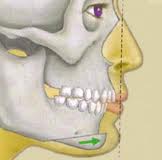 A: There is no correlation between a sliding genioplasty and wisdom teeth, whether they are removed or not. The chin is located on the front part of the jaw while the wisdom teeth (third molars) is on the back part of the jaw. You may be thinking of a sagittal split ramus osteotomy (back of the jaw osteotomy) where having impacted wisdom teeth out six months before the procedure is needed as the embedded tooth roots may interfere with successful splitting of the bone and plate the screw fixation to hold it together as it heals. In fact, wisdom teeth removal can be done at the same time as a sliding genioplasty if necessary.
A: There is no correlation between a sliding genioplasty and wisdom teeth, whether they are removed or not. The chin is located on the front part of the jaw while the wisdom teeth (third molars) is on the back part of the jaw. You may be thinking of a sagittal split ramus osteotomy (back of the jaw osteotomy) where having impacted wisdom teeth out six months before the procedure is needed as the embedded tooth roots may interfere with successful splitting of the bone and plate the screw fixation to hold it together as it heals. In fact, wisdom teeth removal can be done at the same time as a sliding genioplasty if necessary.
A sliding genioplasty is done as a one hour procedure done under general anesthesia in a surgery center not a hospital. The usual total fees are around $6500 for all involved costs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a hairline advancement. I have been looking at your website for a while and you’re the only doctor I’ve found who may be able to perform the surgery I want. My forehead sticks out and bit and I would like to shave it down just a little to make my forehead flatter. I was wondering if this would be possible judging by the images I’ve attached. I’m also thinking I’d like to get my hairline advanced just a little bit. The area I’ve shaded is about the area I’d like to get it reduced to.
A: It is very common for a frontal hairline advancement and a bony forehead reduction to be combined together to create the changes you have shown. You have mentioned that you want just a ‘little hairline advancement although your images show a hairline advancement that I would judge to be up to 10 to 15mms. (which for a hairline advancement would not really be judged as little, that is usually the very maximum that can be achieved in a single stage procedure in just about anyone and even that depends on how much natural laxity of the scalp one has.
What is not very common is to have a male request or to actually do a male hairline advancement. I have done them it, it is just a procedure that is much more commonly done in women. The reason being is that most women have a stable frontal hairline while that is certainly not assured in men. This there is always the concern about placing a fine line scar along a hairline that may or may not be there in the future. While there is no alternative to having an incision to do a bony forehead reduction, there is an alternative (hair transplantation) to a hairline advancement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I think I am interested in a browlift. Recently I have seen major changes to my face. I have been very lucky to always have been told I look younger and more youthful than I am but time has finally caught up with me. As you can see my eyes look tired and I look puffy. I also have always had a duck lip! I tried fillers but as you can see it made it worst. I am looking forward to looking refreshed and as young as I feel. I have started a six month lifestyle change, going to the gym three to four times a week, cutting out sugar and smoking over the next couple of months and studying natural/ holistic food. I feel beautiful until I look in the mirror and I know the potential I could be with a few minor adjustments. I am interested in seeing if you can see this too! I never expect to be a model but would like that twinkle in my eye again. I am looking forward to reviving my youthful look. Looking forward to hearing your suggestions.
A: As all of us age the first changes that are seen are around the eyes. Excess skin develops on the upper eyelids, the lower eyelids become puffy and, for some, the eyebrows drop. Rejuvenation of the aging periorbital region could include upper and/or lower blepharoplasties and browlifts, depending upon which areas are of the greatest concern.
Based upon the one picture that you have sent, it is hard to say what the ideal procedure (s) is for around your eyes since it is only a side view. The upper eyelids shows a little bit of excessive skin, the lower eyelids may actually have some tear troughs and the brows may or may not be low since I have no idea what you looked like years ago. My suspicion is that maybe a browlift and little skin removed from the upper eyelid and fact redistribution on the lower eyelids may suffice…but a few more pictures would be helpful.
For the upper lip protrusion, I would have expected injectable fillers to have made it worse. You would be better served with an upper lip lift which would reduce the protrusion somewhat but also give the upper lip a little more fullness. But again a front view picture would also be helpful in deciding if a lip lift will really be beneficial or not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in ankle liposuction. I am in good shape but have my mothers lower legs:(. No definition between thick ankles and calves) I live in another state so driving in for a consult won’t be possible with 3 small kids. I liked the pics on your site, your work looks great! Just want a ballpark figure so I can see if its in our budget for after the holidays. I can send pictures of my legs, but they are typical cankles. Not large, just not shapely. I run 1/2 marathons and compete in triathlons… Nothing helps give me a calve or smaller ankle. Thanks so much!!!
A: You undoubtably are referring to what is historically known as ‘cankle’ liposuction also known as ankle liposuction or ankle liposculpture. There would not a reason to come in for a consult. Pictures can tell me exactly all I need to know. Creating some definition between the calfs and the ankles is a minor liposuction procedure that narrows the inner and outer ankle widths. The procedure is fairly simple to perform and would cost in the ballpark number of around $4,000. The biggest issue with ankle liposuctiopn is that swelling will persist in the ankle area for awhile and the final result may take as long as three months to see.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question on custom designed facial implants. I had custom designed jaw angle implants made that go from the jaw angle to the chin. I want them placed only through incisions from inside the mouth and no incisions on the outside. My original surgeon said that he could only get them in from an external incision which surprised me. I do not want that scar. Can you get them in from just inside the mouth?
A The custom design method for facial implants is truly amazing when visualized on a computer screen. The ability to create any shape and thickness of an implant and match the symmetry between facial sides, if needed, is impressive. But one limitation of computer designing implants is that it is done on an inanimate facial skeletal computer image that does not take into account the soft tissue cover…nor how such designed implants may be capable of being placed. Given that placing facial implants must be done in an inconspicuous and visible scar-free manner, being able to get a custom designed implant through the limitations of intraoral or discrete external facial incisions can be problematic.
Custom designing facial implants often allows larger and more encompassing implants to be created. But part of their design must take into consideration how they can be inserted and whether the overlying soft tissue cover will be adequate and still get the incision closed in a tension-free manner over it.
I have found it useful in many custom designed facial implants to have them sectioned or cut up into smaller implants so that they can be inserted from just inside the mouth. All sectioning the implants does is enable them to be placed through intraoral incisions. It does not affect the accuracy of their placement and, in some cases, may actually make them more accurately placed. One of the things you learn by doing a lot of custom implants over the years is that anything can be designed on a skull model or a 3D scanned image. Whether they can actually be placed (inserted through the limits of the incisions) and with good soft tissue cover, elements in the surgery that are often more important than the design for an uncomplicated result, is often another matter and must be considered beforehand to avoid an unpleasant intraoperative surprise.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a questions about gummy smile surgery. I am a 25 year-old female. I have an upper jaw prominence as well as a gummy smile. It shows 8 mm of the gum. I went to a dentist to do a lowering lip surgery, however, he said that even if he would do it for me the gummy smile will go back once more time because of the upper jaw prominence. I end up thinking what if I do a V-Y flap or a W technique for upper lip lengthening?. Are they going to work in my case and last for good? Or there will be a relapse because of the upper jaw prominence. I hope you get my point. Thank you.
A: When it comes to gummy smile surgery, the potential for relapse is related to the surgical technique not how much upper jaw prominence one has. The key to preventing relapse in upper lip lengthening is the vestibuloplasty portion of the procedure. Shortening the depth of the vestibule will serve to keep the upper lip from relapsing back to original position. Going to a dentist is probably not the best doctor to have treat a gummy smile that is so excessive which is probably beyond their comfort zone and experience.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have linear scleroderma which affects my forehead and would be interested in discussing how it could be treated. I’m 44 and balding, so the scar is much more prevalent than it had been when I had more hair. According my doctor out here, it’s burned out. I’d like to learn more about your experience with this problem and how you might look to correct it.
A: Your linear scleroderma involvement of the forehead and scalp is fairly classic, going down (or up) along the pathway of the 1st division of the trigeminal nerve. At your age it would be fairly common that the disease process has burned itself out. There are numerous approaches to the reconstruction of the aesthetic forehead defects from it, most of which focus on volume restoration using various forms of fat grafting. The problem with that exclusive approach is that it can not restore the quality of the overlying skin which is usually thinner and discolored to some degree. Even with volume enhancement, the vertical orientation of the involved skin is still very apparent.
In your linear scleroderma case, I would use two different surgical techniques which are different. On the forehead, I would excise the entire length of the involved skin and put the closure back together in a broken line closure methods due to the numerous horizontal wrinkle lines that you have. This would be an ideal way to really hide the scar well. This would not only ensure a permanent and assured resolution to the forehead soft tissue defect but also gets rid of the deformed skin. On the scalp, however, a different approach would be used as it is smooth skin with no wrinkles lines to help hide the scar. I would do fat injection grafting to restore the indentation only.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in liposuction or perhaps one of the non-invasive body contouring approaches. I am a petite 23-year old female who is 5’4” tall and weights 112 lbs. I am in pretty good shape, but have areas of fat on each of my inner posterior thighs that will not go away with any form of exercise and have been there all my life. I would be very happy with a visible reduction of this area and the bulges eliminated. I am also very apprehensive about any procedure requiring general anesthesia and would greatly prefer to reduce risk. But on the other hand, I don’t want to waste money on noninvasive treatments that don’t offer a significant improvement.
A: Liposuction would be the most efficient and effective method of fat removal for your inner thigh areas. But given their small size, this could be done under local anesthesia with or without oral or IV sedation if you were so motivated. While Coolsculpting or Exilis devices would produce some positive changes in the inner thigh bulges, it would not be as much nor as fast as with microcannula liposuction fat extraction. Since these inner thigh bulges have been present your entire life and this body area is not a known fat depot side, the reductive changes induced by liposuction should be permanent.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a natural breast augmentation that will last and hopefully not need to be redone repeatedly. Also, I can not support stem cell enriched augmentation if the source of such cells is from aborted babies. Is this the only source? What is being done such as in other countries? I am also wondering about the possible risk of cancer cells growing from such a procedure. The only info I could find about that seemed to be related to women who had the procedure following a lumpectomy or mastectomy.
Do you recommend the fat transfer procedures? I am not comfortable with the silicone or saline options because of the risks.
I am very small busted and have breast fed many children and now have nearly nothing left.I was small to begin with and now that my last baby is weaned, it is quite different than lactating. Thank you for the information.
A: What you are seeking in natural breast augmentation is the holy grail…natural, permanent, and does not involve an implant. By today’s techniques, you are seeking something that does not yet exist. Natural breast augmentation today uses one’s own fat that is processed and then injected and may have some viable stem cells in it. Besides having to have enough to fat to harvest and use, one has to accept the unpredictability of how much fat will survive and whether it survive smoothly without irregularites. There is also the risk that the procedure may have to be repeated depending upon how much fat survives during the first procedure. What is not known about fat transfer is if it increases the risk of breast cancer although this is believed to not be a concern.
While fat injection breast augmentation is done today and is becoming more mainstream, it is still restricted to a very few women who have the right physical qualifications for it. It is far from a breast augmentation technique that is perfected. For a reliable breast augmentation result that produces an immediate and predictable result, implants a much more reliable technique despite the limitations of being a medical device.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull reshaping for a flat spot on the back of the head. My son is twelve and has a noticeable flat on the back of the right side of his head. He has not said anything about it yet. In preparation for the possibility of coming to see you, I have an important question. Does getting kryptonite mean he will never be able to play contact sports such as football again?
A: Skull reshaping that involves building out flat or depressed areas is done by applying a bone cement material on the outer aspect of the skull. In answer to your specific question, kryptonite as a cranial augmentation material is no longer available and has not been so since late 2011. In answer to your general question, augmentation of the occiput (back of the head) would in no way preclude one from participating in form of sporting activity including contact sports. The strength of the cranioplasty material up against the rigid skull bone makes for a very hard construct that has the same strength as that of natural skull bone. This makes it highly impact resistant to the infrequent contact to the head that may occur in most sports.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How can I be a part of the FDA-approved clinical study for stem cell enriched breast augmentation?
A: To the best of my knowledge, there is no current FDA study that is evaluating stem cell enriched breast augmentation. Some plastic surgeons use the term ‘stem cell enriched’ when breast augmentation is done by fat injections, but that is neither part of an FDA sanctioned study nor is it truly stem cell enriched. Since all harvested and processed fat contains stem cells, calling fat injections stem cell enriched is a very liberal use of that term. (more bluntly an exaggeration) True stem cell enrichment would mean that stem cells are isolated and then put back into fat injections in a very concentrated form with high numbers of active cells. That is a quite different process that simple fat harvest and concentration.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to have double chin surgery. I am just 42 years old and have a roll of what feels like fat under my neck that never goes away. I am actually very slim and this is my only problem area on my entire body. What treatment is recommended in my case? Thank you.
A: The type of double chin surgery that one needs must take into account four anatomic factors. How much fat is in the double chin? Is the chin short or has inadequate projection? Is the plastyma neck muscle separated or split apart allowing deep fat to protrude through? Is the neck skin loose? This corresponding treatments could include submental/neck liposuction, chin augmentation, a platysmaplasty or a full necklift.
For a patient in their early 40’s who is unlikely to have much loose skin (unless you have lost a lot of weight) the most likely anatomic culprit is fat, making liposuction a primary treatment. If you have a weak chin, a chin implant will significantly help with the liposuction with a diametric benefit to the jawline. (neck goes up, chin comes forward)
If you have a very heavy neck, a playsmaplasty (tightening the neck though a small incision underneath the chin) will improve the angle of the neck more than liposuction alone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a breast augmentation revision. My original breast implamt surgery was about a year ago. I feel like I paid to have big saggy boobs. I wanted a “fake” look and I don’t think my doctor was listening to me. When I lay down they fall to the sides. I have saline implants (500ccs overfilled) under the muscle. I have three kids so they were deflated beforehand and a little saggy. They don’t look horrible now but they are not what I wanted. I waned a very full upper. I think they look natural and I don’t like that. Attached are some pictures of my breasts from today.
A: In breast augmentation revision, it is extremely important to know from where you and where you want to go from here..and then determine if it is realistic and how it might be achieved. You obviously had some significant sagging beforehand so the implants have merely taken what you had and make it bigger…filling out the deflated breast mound. This leaves you with larger breasts that still have some sag and not the upper pole fullness that you want. You have three options for a breast augmentation revision. One is to simply place bigger implants. With indwelling 500ccs implants (let’s say 550 since they are overfilled), it would have to be a minimum of 250cc size increase to be significant and ‘fake’ looking. Even bigger implants will not lift up your breasts higher on your chest wall. This approach just gives you bigger breasts that through a volume increase would provide some greater upper pole fullness. The second option would be to keep your current breast implants and do a lift, putting them higher-up on your chest which would make them look rounder and higher. This will create scars to do so and would be challenging to do with your tight skin and keep your current size implants. Given the current shape and position of your breasts, the prospect of scars on your breasts does not seem justified even though they are somewhat low and still a little saggy. Lastly, you can just aim to keep them from falling to the sides so much.You can tighten the pocket (lateral suture capsule tightening) to keep them from falling to the sides. This would only improve but one problem that you currently see in your breast augmentation result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a skull reshaping. I am a 32 year-old man with an odd-shaped head with a prominent ridge running own the middle. While I could always feel it, it never bothered me until I started to lose my hair. Now I feel like an alien with this visible ridge on my skull. Can it be reduced?
A: Skull reshaping can involve reduction of prominent bony areas or bony buildup of deficiencies. One particular bony skull excess is the sagittal ridge or crest that occurs in the midline of the head. It usually occurs due to a mild anomaly of how the sagittal suture closes after birth. As a result it can develop excessively thickening creating a ridge or crest in the midline of the head that is especially noticeable in men that have short hair or shaved heads.
Because it is a bone protrusion or thickening it can be reduced to a more normal skull contour without risk of exposing the dura or penetrating into the brain. This procedure is done under general anesthesia through an incision placed at the back end of the crest. A scalp flap is elevated exposing the crest that is reduced with the use of a burr creating a smoother upper skull contour. The scalp tissue is closed without use of any drains and only a head dressing is used for the night after surgery after which it can be removed. These small scalp incisions can heal remarkably well.
In summary the sagittal ridge is a midline bone protrusion that can be reduced through a minor skull reshaping procedure using small scalp incision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting pectoral implants to make my chest bigger. My two very important questions are does the implants distort upon muscle contraction when placed under the muscles? And to create the “pocket” for the implant you need to detach the muscle from the sternum right? Thanks for getting back to me.
A: While there are some similarities between pectoral implants and breast implants, there are difference between them that are more just that one is for men and the other is for women. The implants themselves are different with pectoral implants being a soft but solid silicone elastomer while breast implants are filled with non-solid fillers inside a thin flexible silicone elastomer bag. As such, breast implants can fail and need to be replaced while pectoral implants can not fail and never need to be replaced.
Pectoral implants are put in through an incision in the armpit (just like some breast implants are) and are placed in a completely submuscular pocket. Conversely, breast implants are placed in a partial submuscular pocket often referred to as a dual plane location (part under the muscle and part out of the muscle. When you think of implant distortion with muscle contraction you are thinking of breast implants where half of the implant is not under the muscle and thus distorts when the muscle pushes down on it, causing the implant to move to the side and causing some degree of implant distortion/movement. Neither in breast or pectoral implants is the muscle detached from the sternum at either its origin or insertion. The pockets are created by entering a tissue plane underneath the pectoralis major muscle.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in skull reshaping of the back of my head. I am 45 years and I have a small spot of protruded ridged edge at the back of my head from birth. I have never been comfortable with it and I wish it could be corrected for a normal round shape back head. I wish to know if/how it could be corrected. If possible, what’s the cost implication and how the duration of the treatment and possible medical implications if any. I have attached some photos for your examination and prompt response, I may send you more pictures if you so request. Thanks.
A: Your head problem could be solved by a minor skull reshaping procedure. Your ‘spot’ or bump of bone on the back of your head is a raised area over your original posterior fontanelle area that you had an an infant. This is a common area of minor skull contour deformities from indentations to raised ridges. Your midline occipital ridge can be reduced by a burring technique through a small incision. This is a one hour procedure done under general anesthesia as an outpatient procedure. There are no medical implications by taking a small amount of the outer cranial table. Other than some temporary swelling and small fine line scar from the incision there are no potential complications.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in extra large breast augmentation. (technically extra large breast implant replacement. Can we do a consultation via email since I live far away. I want 1000cc implants. I currently have 500cc on right breast and 400cc on left and clearly they are not even close to being as big as I asked for. The dr was more concerned about doing what he thought looked best and not accommodating what I wanted at all. It is humiliating as they look awful. This is not remotely the size I was looking to get.
A: The concept of extra large breast augmentation is controversial amongst plastic surgeons. There is a large group of plastic surgeons who choose breast implants based on their assessment of the breast tissues to support them over the long-term. With this concept they do not put sizes that are wider than the patient’s natural breast base diameter or the less measurable quality of the support of the overlying breast tissue/skin sleeve. For many patients this means that sizes less than 400ccs are placed. There is another group of plastic surgeons, arguably smaller, that provide any breast implant size that the patient wants including very large sizes. These implant sizes do irreversibly stretch out the breast tissues and are more prone to bottoming out over time (loss of support) but do meet the patient’s expectations.
What your initial breast augmentation result was less than you wanted, your plastic surgeon probably placed implants that he felt comfortable could be adequately supported by your breast tissues. He or she was looking out for some long-term issues that most patients are understandably not aware of. This may have been too conservative for you but was a safe approach. The good news is that this is an improveable problem, albeit with another surgery, and larger implants can be placed. You also have the advantage of now knowing what implant size may be acceptable since you know what size change has occurred with the volume you now have in. It is now about volume ratios. If you want a breast size that is twice as big as you now have, you will need a 100% increase in the implant’s volume.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in learning more about the forehead reduction (hairline lowering) surgery. I genetically have a very high forehead that I’ve always been very self-conscious about. I’m just now learning this surgery exists! I live out of state, so I can’t easily come in for a consultation. How do you handle out of town patients for consults? Can you just use the photos? With that, I’d also like to know the approximate cost of this surgery (or can you estimate based off pictures?). I would appreciate any information you can provide, and please let me know what other information I can provide to you. At this time, email is the best way to contact me. Thank you, and looking forward to hearing back from you!
A: Forehead reduction surgery can be beneficial for those women that have a long forehead, which almost measures greater than 6.5 cms from the eyebrow to the hairline. Vertical forehead reduction is a skin operation where forehead skin is removed along the hairline and the scalp is advanced in its place. This requires an incision along the frontal hairline and is very much like a reverse pretrichial browlift. The success of the procedure is primarily based on how much natural looseness the scalp has and how much can be surgically created. It is this looseness that allows the scalp to be brought forward. Generally about 10 to 15 mms can be gain in most patients. If the scalp is very tight or the amount of scalp advancement needed exceeds 15mms, then a first stage scalp tissue expander needs to be placed. You can determine how much scalp advancement is needed by taking a mascara pen or lip liner and drawing a line where you want the new frontal hairline and measuring it. Also remember that the greatest amount of scalp advancement is in the middle and becomes less so as it tapers to the sides into the temporal scalp.
We have many far away patients and further discussions can be done by phone or a Skype video consultation. It is not necessary to come in for a separate in-office consultation. The cost of the surgery is very similar to a pretrichial browlift, as I have mentioned, and my office will pass along the cost to you in a separate e-mail in the next few days.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in forehead reduction surgery. I serve in the military and I really want this forehead reduction done. I hate my forehead. It is wide with a high hairline and my forehead protrudes. Please help me! I would love to do the military program but this procedure is not on the list. Attached are some photos which shows how high my hairline is and how my forehead bulges out.
A: While you would be a good candidate for a forehead reduction or scalp hairline advancement, it appears you would need almost a 2 cm advancement given the length of your forehead. This means a first stage scalp tissue expander is placed to create more hair-bearing scalp that then can be used and advanced to create a really significant forehead reduction as a second procedure. Without a tissue expander or a two-stage approach, the most hairline advancement that can usually be obtained is around 1 cm. While forehead bone reshaping would be also be done, the forehead always seems to stick out more when the hairline is way high and the upper forehead is sloped backwards. Even a hairline advancement procedure alone make a prominent forehead look less protruding because its total vertical length becomes less.
The Patriot Plastic Surgery program applies to all elective aesthetic plastic surgery procedures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting a chin augmentation surgery. I have attached a couple of photos in order to get your opinion. You had written that there is a permanent chin augmentation solution where the implants are secured by small titanium screws. Would those screws need to be replaced after ten or more years? Do they set off metal detectors? It seems that screwing the implant in makes more sense. As my chief concern is the security of the implant and its ability to withstand an occasional stiff impact. I do know some chin implants are used without screws. What is your opinion on those types? My feeling was that since they are just placed on top of the chin and not secured with anything the likelihood for them to become dislodged increases. Not sure if that is true though. Assuming that there are different types of chin implants, (some more square, some more rounded) perhaps when you see the attached photos you’ll have a better idea which one would benefit me the most. Finally, I would be remised if I did not say that being your office is in Indianapolis it seems difficult that I would fly from another state for such a procedure. The logistics alone would be difficult to for me to work around. Though being your reputation is excellent, nothing is completely out of bounds. Thanks for your time, it is very much appreciated.
A: Your photos demonstrate that you would be an excellent candidate for chin augmentation. Your chin deficiency, compared to many patients that I treat is relatively mild, but I would agree that more chin projection and a more square chin appearance would have some aesthetic benefits for you. I will do some computer imaging of that and send it to you later today.
In answer to your questions about chin implants and screw fixation, this is a technique that I have always done in the vast majority of chin implants. It is simple, quick and inexpensive to do and assures that for the lifetime of the patient the chin implant is never going to move or become dislodged. I have certainly never seen it in the 25 yeasrs that I have been doing the procedure. The screws are composed of titanium, a pure element that never degrades or corrodes or needs to be replaced. It is a non-ferromagnetic metal, which means it does not set off metal detectors nor affects MRI scans. While placing screws is not standard practice for most surgeons that place any type of facial implants, it really should be.
While being a far away patient may seem unusual, it is standard in my practice as patients fly in from all over the world every week for surgery. It is easier to do than you think and handling the logistics of how to do it efficiently is a common occurrence for my staff and surgery center.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m undergoing a breast augmentation in less than a week and I like the look of your case study, breast augmentation in Asian women. I am exactly her size except a smaller breast base diameter (10.5). For reference, what profile is the implant you used? I would appreciate any info you could give me. Choosing between 260 high profile, 280 high profile, or 320 full profile (leaning toward 280).
 A: Many patients get hung up when considering their breast augmentation of an implant’s profile which actually has little to no influence on the final breast shape, contrary to popular perception. The only real relevance to an implant’s profile is how it influences the base diameter with the goal of using an implant whose base diameter is no larger than one’s natural breast base width. This is the real role of high projection/profiled implants, keeping the desired volume in a very narrow chest to within the breast dimensions. Almost assuredly with a breast base diameter of only 10.5 cms, any implant volume over 225cc will need a high profile implant to accomplish that important aesthetic goal.
A: Many patients get hung up when considering their breast augmentation of an implant’s profile which actually has little to no influence on the final breast shape, contrary to popular perception. The only real relevance to an implant’s profile is how it influences the base diameter with the goal of using an implant whose base diameter is no larger than one’s natural breast base width. This is the real role of high projection/profiled implants, keeping the desired volume in a very narrow chest to within the breast dimensions. Almost assuredly with a breast base diameter of only 10.5 cms, any implant volume over 225cc will need a high profile implant to accomplish that important aesthetic goal.
Not to confuse you further, as the implant manufactures do a good job of that in this regard anyway, there is no correlation between any of three manufacturer’s (Allergan, Mentor and Sientra) implants in regards to volume and their profile types.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Liposuction of the Dorsocervical fat accumulation. I am curious if you do this procedure and what ball park of cost would this procedure be in. Please advise as I need your help.
A: Liposuction is an excellent option and often preferred treatment for neck fat. I believe when you refer to the dorsocervical fat accumulation, you seek the classic ‘Buffalo Hump’ reduction. This is a procedure that I have done numerous times (most commonly in the HIV patient although not always) and I have found that the use of laser liposuction (Smartlipo) can give a very effective reduction without the need for an open operation with a long incision. This is a procedure that takes less than an hour to do, often under sedation or general anesthesia. (it is helpful to have the patient have a good anesthetic depth so the liposuction procedure can be aggressive) Buffalo humps consist of a very fibrous type of fat (often looking more white than yellow) as opposed to a softer and more buttery type of fat more commonly seen in many areas of the body including the anterior neck. This is why laser liposuction or power-assisted liposuction (PAL) is used as it is more effective at breaking up this more dense fat that is held together by fibrous tissue bands. Buffalo humps can be very effectively reduced by this liposuction approach. In my experience, patients have not reported a recurrence of this posterior neck fat accumulation. The ballpark cost would be in the $4,000 to $4,500 range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been trying to get an abdominal panniculectomy since I lost so much weight. My insurance company denied me but I plan to appeal. I have infections and skin ulcers. It makes it hard to do my job. I heard about the Patriot Plastic Surgery Program and wondered if you can help. PLEASE!!! I wanted to get this done before my husband got home from his latest deployment and I was wanting to get this done before he got home and I’ve run into roadblock after roadblock. Can you help? I have attached some pictures of my abdominal problem.
A: While there is little doubt that you would benefit from an abdominal panniculectomy, I am not surprised that you have been denied by your insurance company. By insurance requirements you do not meet the very basic criteria of the size of the pannus, it must reach down and overlap onto the thighs. Plus there must be a 6 month history of medically documented skin infections that have failed to respond to topical therapies and there must also be current photographic evidence of active skin infections. Failure to meet all of these criteria will result in denial of coverage for an abdominal panniculectomy. This is a very common occurrence and can be difficult to appeal without providing documentation of their established criteria.
The Patriot Plastic Surgery program is where some reduction in fees is offered for a variety of cosmetic surgery procedures, including tummy tuck and abdominal panniculectomy.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am wondering if scar revision can help? I have had this one inch long scar in my eyebrow frown line since I was a toddler. Because of its location it is starting to become more noticeable as I approach 30. I have tried Botox, SmartXide laser, TCA Chemical Peels, and Sciton LaserPeel and not been that satisfied with the results. I was wondering if you thought it could be improved with a revision or dermal filler or if you think it should just be left alone. The indentation is my primary concern vs. the white line color. Looking forward to hearing from you!
A: Given the effort that you have made to improve your forehead scar, it is reasonable to consider surgical scar revision at this point.That scar is perfectly oriented in exactly where vertical glabellar wrinkles develop. That is why it has been getting more noticeable as you age because it probably is deepening slightly with repeated expressive motions. I am not surprised that none of the treatments you have had were successful as the depth of the ‘crease’ is beyond what they can level out. You are correct in assuming that scar revision would be the only successful approach. An injectable filler will lift up the depression as the skin edges are tethered down. A small geometric broken line closure scar revision would both release the scar contracture, elevate the scar and rearrange the skin edges by interdigitation to prevent recurrence.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in getting a breast reduction done but I would like to know if I can breast feed later on when I decide to have children. I am 25 years old, size 38DD, with a height of 4′ 11”. I have been having a lot of back pains,shoulders, and even neck pain as well. This is why I am interested in breast reduction.
A: Breast reduction is a commonly performed procedure that is frequently done in young women who have not yet had children. Even though it is a breast procedure that involves the glandular tissue, it does not interfere with the ability to breast feed. Many women have had breast reduction that have gone on to have children and were able to breast feed successfully. This is because the nipple-areolar complex and its attached ductal tissue remains intact to the central glandular breast mound which is not disrupted from its vascular attachments to the pectoralis fascia/muscle. Thus breast milk can be made and delivered through the uninterrupted and unscarred ducts out through the nipples. The incisions that one sees on the breast mound after a breast reduction have no connection to the breast lactation system.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i am interested in nano fat grafting. I have heard that fat is beneficial to scar contracture but also I am aware that fat won’t survive in a scar bed and I could wind up with lumps. That is why I thought that the nanofat probably won’t do any harm and may even help. The side of my nose that has a depression or drop off angle is the area with the scar tissue build up. The tissue is parchment thin there. I would like to fill this area with an autologous material. I had surgery 3 years ago to revise a rib graft done nearly 6 years ago which left me with unatural harsh drop offs on either side of my bridge. I already had restylane done last year and it lumped up on me and caused too much pressure in my nose. I have also been considering trying belotero filler, Would you have any suggestions?
A: While I think nano fat grafting would not hurt, I don’t think it will produce any positive benefits in terms of filling in skin depressions or rib graft step off areas. This all would be better served to be filled with alloderm (allogeneic) dermal grafts.
There is a difference between scar tissue build-up (contracture) and trying to make the skin thicker or fill in contour depression areas. If the rib graft not has sharp edges or visible stepoffs,, adding a layer of alloderm or been temporalis fascia would be the more assured way of improving the soft tissue cover.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a rhinoplasty to permanently build up my radix. I had some fillers placed in my radix and glabella a few months back, and I really liked the augmentation. Anyway, I’m intending to get a rhinoplasty to augment these areas permanently next year. As such, I was wondering if it were possible to do so and if so, what kind of material will be used? I understand that rib grafts are used for the bridge, but can it also be used for the radix/glabella? Secondly, I’m hoping to get a touch up with some fillers some time in December. Will it be fine for me to do so, or will repeated treatments of dermal fillers complicate the rhinoplasty?
A: A radix augmentation rhinoplasty can use either autogenous or synthetic materials. But, in my opinion, cartilage grafts are the best material to use for radix augmentation. They will hold up for the rest of your life without any risks of complications. The size of the radix defect and the volume needed will determine where the cartilage should come from. (i.e., donor site) While rib cartilage is always ideal in terms of unlimited volume, most radix augmentations can be done with septal or ear cartilage the vast majority of time. There is no problem with getting fillers again next month. It does not complicate placing a radix cartilage graft later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My question is in regards to the safety and security of chin implants. While I firmly believe such a procedure would improve my appearance my hesitation lies in the uncertainty of the implant being a permanent solution. To be specific my job is such that at times is of a physical nature and am worried that the implant could become dislodged. How is it kept in place? And are there certain implants designs that are better then others? Would hard impact to the chin or jaw cause it to become dislodged? Perhaps you know people in the Military who have had this done? My second line of questions are about the health risks of a foreign element placed in the body. Are there long term effects from having a implant inserted and is this something that once done should remain for life? Thanks for your time.
A: Chin implants, almost of any implant placed on the body, are the safest (less likely to have complications) in my long plastic surgery experience. There are a permanent chin augmentation solution as the material will never degrade. The implants are secured in place by small titanium screws so that they will never move or become dislodged. I have yet to have a case where a chin implant became dislodged or displaced because of trauma of any nature, including patients in the military. There are no health risks from performed silicone since it is a molecularly stable material that does not degrade or release any free silicone molecules.
Dr. Barry Eppley
Indianapolis, Indiana