Your Questions
Your Questions
Q: Dr. Eppley, I am a 35 year-old male who is interested in jaw angle implants. It seems to be hard to find surgeons who do this procedure with any regularity or expertise in it. I’ve met many surgeons during the last three years and none seems to be expert in it. I know the distance could be a problem in case of complications, but I’m financially ready and, if I remember well, we talked a couple of years ago on another website about this procedure. I had a rhinoplasty and chin implant back in 2010 (conform extended anatomical chin implant, size large, Implantech) and I really would to go on with the work on my face having jaw angle implants.Do you work on international patients? And are two weeks there enough to fly back safely? I see my face as very vertical, so I think I would only need width and not add further vertical projection.
A: I would certainly agree based on your pictures that you only need width enhancing jaw angle implants and not vertical lengthening ones. While the surgery does cause some swelling I would see no need to be here any longer than 5 to 7 days at most before flying home. Fortunately any serious complications are very rare (e.g., infection) so being at a great distance is rarely an issue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in possibly getting cheek and chin implants (or starting out with dermal filler) to attain a more chiseled & angular look. I would like to get a well-defined, hollowed-out appearance similar to what many actors have.
I am especially interested in seeing if I can obtain not just the hollowed-out cheeks, but also the well-defined line that seems to run from the cheeks to the chin on both sides of his face (this effect is especially noticeable in the last picture).
I have also submitted two photos of myself; please excuse the eye asymmetry, which occurs occasionally due to an outdoor allergic reaction (I run/jog outside a lot).
Generally speaking, do you think the goals I am trying to achieve are realistic?
A: Based in these pictures and your face, I do not find your facial goals especially realistic. While cheek and chin implants will help create more prominent facial structures, they will not necessarily cause that hollowed look you are seeking. That is caused as much by the lack of any subcutaneous fat over the trampoline area of the face and prominent jaw angles as it is caused by any prominent cheek and chin structure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently undergoing orthodontic treatment to correct a severe overbite which has also caused a recessed chin and weak jaw. My orthodontist said it may be necessary to undergo orthognathic surgery following my treatment. While I’m perfectly happy to do this, there is a good chance my insurance won’t cover it as it is not causing a medical problem (such as sleep apnea or speech impediments) and the surgery can cost anywhere from $20-50k.
I want to know if a custom wrap around jawline implant could give the same aesthetic effects of the jawline (fix my recessed chin/weak jaw) as orthognathic surgery of the mandible? In other words, can the implant mask the appearance issue of the jawline without actually addressing the functionality issue of an overbite?
A: The simple answer to your question is yes. In reality, a custom wrap around jawline implant offers much more versatility in terms of dimensional facial changes than any form of orthognathic surgery. A sagittal split osteotomy advancement of the mandible can really only supply a horizontal forward movement whose limit is based on the difference between the pre surgical relationship of the upper and lower teeth.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, what can I do to make sure my breasts won’t be too far apart after getting breast implants? I know that breast augmentation doesn’t change where your natural breasts sit and that it only enlarges them. But I simply don’t want my new breasts to be too far apart. What can I tell my surgeon to make sure that my breasts are full and close together?
 A: You are both asking a reasonable question abut a common breast augmentation concern and also answering it at the same time. You have correctly surmised that all breast implants do is make your natural breasts fuller. That may or may not necessarily make them somewhat closer together depending upon the size of the implants. But there is no guarantee that they will and there is not anything your surgeon can do to change the natural wide spacing between your breasts. You will need to accept that this is a limitation of breast augmentation surgery and is a function of your anatomy and not your surgeon’s technique or ability. At the least, every plastic surgeon recognizes and understands this implant spacing concern…and usually goes to great lengths to point it out and that your after surgery result is still going to have a sternal gap between the augmented breasts.
A: You are both asking a reasonable question abut a common breast augmentation concern and also answering it at the same time. You have correctly surmised that all breast implants do is make your natural breasts fuller. That may or may not necessarily make them somewhat closer together depending upon the size of the implants. But there is no guarantee that they will and there is not anything your surgeon can do to change the natural wide spacing between your breasts. You will need to accept that this is a limitation of breast augmentation surgery and is a function of your anatomy and not your surgeon’s technique or ability. At the least, every plastic surgeon recognizes and understands this implant spacing concern…and usually goes to great lengths to point it out and that your after surgery result is still going to have a sternal gap between the augmented breasts.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a very narrow, dolichocephalic skull shape and I would like to increase the width of my head. According to the information on head widening provided on your website there are two options to achieve this:
1. Augmenting the posterior part of the temporalis muscle by injecting fat.
2. Placing an implant under the temporalis muscle above the ears.
I prefer option 1 since I would like to avoid implants. However, if the achievable results of fat injections are unsatisfactory I will gladly consider alternatives.
Thus I have the following questions:
1. By how many millimeters can the head be widened through fat injections to the posterior aspect of the temporalis muscle? Are 5mm per side achievable?
2. How much would the procedure cost if i) only the posterior part and ii) both the anterior and the posterior part of the temporalis were to be augmented?
3. How much does it cost to widen the head using semi-custom-made implants with a thickness of 5mm per implant?
4. Are there any other methods to increase the head without producing visible scars?
Thank you for your time.
A: The short answer to your question about head widening through posterior temporal augmentation is that only an implant is going to consistently work. The first issue with fat that you have to have enough to harvest, process and then inject. In a thin person, which it appears you are, that could be the rate limiting step right there. No matter what is injected only a fraction will survive and what survives most certainly is not likely to be symmetric.
The use of a semi-custom temporal widening implant is assured, can easily increase the side width by 5mms and is placed through an incision that is limited to the back of the ear. (thus being placed in a scarless fashion) Any consideration of fat injection use should be limited to the temporal hollowing located next to the eye area (anterior temporal augmentation) where a more posterior implant does not reach. There are very effective implants for that area as well but they require a more exposed vertical incision in the temporal scalp region.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How long should I wait to have a tummy tuck after having a baby. I delivered my baby three months ago and I am now very close to my before pregnancy weight. I am only about 3 lbs from it at this point. The issue is not the weight but the ton of loose skin that I have. I know that I am not going to have any more children so I am ready whenever a doctor says I should do it. I also have a lot of stretch marks which I really don’t like, will a tummy tuck get rid of all of them? Lastly, what type of tummy tuck should I have… a full or mini tuck?
A: The typical answer from most plastic surgeons is that the earliest that a tummy tuck should be done after a pregnancy is six months. This gives a woman ample time to lose as much as of their pregnancy weight as possible and to be able to take care of a new babcy before embarking on a need for their own recovery. It is also important to remember that this is an elective procedure so any need to rush the decision for surgery is an emotional one not one of medical necessity.
By using the term, ton of loose skin, this implies that a full tummy tuck is needed for the best result. This form of a tummy tuck is also the most assured way of getting off the maximum number of stretch marks. While it does result in a longer scar, the result is always better than when less tissue is removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have several questions about vertical chin lengthening. They are as follows:
1) Given my case of wanting vertical elongation with some minimal horizontal projection, are my needs best served with a chin implant or a sliding genioplasty and which one in your professional opinion would you recommend and why?
2) I am primarily interested in a sliding genioplasty and would prefer to avoid an implant. In my case, would you be willing and able to do a sliding genioplasty on me instead of an implant?
3) Can vertical elongation be achieved with a sliding genioplasty?
4) With a chin implant, can vertical elongation be achieved?
5) I noticed that when I smile, my chin seems to jut out. However, upon closer observation, I noticed that it is because my entire face goes upward when I do smile. Would A chin implant emphasize this jutting out of the chin?
6) What a sliding genioplasty emphasize this jutting out of the chin as described above?
7) Since my chin seems to jutt out when I smile, it is possible for a sliding genioplasty to be done primarily for vertical elongation purposes and minimal forward movement?
8) Do you think I would have mentalis muscle strain with a sliding genioplasty?
9) If a sliding genioplasty is done, is there a chance that my lower lip might not be able to touch upon the top lip and would struggle to close my mouth? Is this is same as mentalis muscle strain?
10) Will the lip curl of my lower lip downward be exaggerated with a chin implant given that a chin implant primarily is done for horizontal projection and not for vertical elongation which is my goal?
11) With a sliding genioplasty, because the bone would be brought down and slightly out, will that create a more v-shape/heart shape look to my lower face?
Thank you so much Dr. Eppley and I look forward to your response.
A: In answer to your specific questions:
1) For pure vertical chin elongation, either a sliding genioplasty or a chin implant can be used. But the chin implant would have to be custom made to achieve a vertical lengthening since they are not manufactured in standard shapes to normally do so. I have done in either way for various patients and their affinity or disdain for an implant will determine the choice. Most, if not all, Asian women that I have treated or discussed this type of chin change are going to opt for a sliding genioplasty approach.
2) Your preference for a sliding genioplasty indicates that is the preferred choice for you.
3) Vertical elongation alone can easily be achieved with a sliding genioplasty.
4) Only a custom chin implant can achieve vertical lengthening.
5) and 6) Neither a chin implant or a sliding genioplasty is going to make this jutting out of the chin change. Whether it would make it worse can not be predicted.
7) A sliding genioplasty can be done in any dimension one wants. While it may be commonly done for horizontal advancement, that does not mean it has to be done for that movement. You seem to be under a misconception that it is somehow unusual or difficult to just move the move for vertical lengthening alone when it is not. That is the easiest movement to make for a sliding genioplasty.
8) Any change in the bone position of the chin runs the risk of creating a mentalis strain. It is not very common but potentially can happen.
9) Lower lip incompetence and mentalis strain are indeed related. Again it is not a very common problem to occur after a sliding genioplasty but is possible.
10) Since you are not interested in a chin implant, this question does not seem applicable.
11) Vertical lengthening of the chin by a bony genioplasty is a well known facial bone technique for making the face more heart shaped. This can be particularly aided by also narrowing the chin bone as it is lengthened.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What I most dislike about my face at this time are the bags/creases under my eyes that make me look tired and old. There are also some fairly “deep” lines in my forehead. I am turning 35 next month, so I don’t think I want any type of surgery yet. I am interested to find out what types of options there are for me and what it might cost. Likely, I would do this in the spring time over school break. Thanks!
A: The earliest signs of facial aging always with exactly what you are seeing. Wrinkle lines on the forehead and/or around the eyes and the development of bags (herniated fat ) on the lower eyelids. Botox injections work well for forehead wrinkle lines. Lower eyelid bags are really best treated by removal. (transconjunctival blepharoplasty) But to those adverse to surgery, injectable fillers can be used to fill in the tear troughs created by the bags. Such injection treatments in my experience are a mixed ‘bag’ since they have a not rare problem of lumps and unevenness due to the thin skin of the eyelids. When they work well they are great but when irregularities develop the filler often has to be dissolved away by hyaluronidase injections.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi. I have about a half inch of bone loss in my parietal regin going all the way to the back of my head and bone loss in my back of my head. I saw that you performed an implant on some with a similar problem with silicon. I wanted to know if there was anything else available because I don’t feel comfortable about putting silicon in my body. Would fat transfer work or would you recommend something else. I have had this problem for years, but hair is thinning out and I am not able to cover it up like I used to. Thank you!
A: There are lots of different materials that can be used for skull augmentation or fill in of defects.The one major issue with all of them is that wide open exposure is needed to apply them to the bone site. In other words, a long scar across the top of your head. The reason that custom silicone implants are one of the most popular forms of skull augmentation is that they can be placed through much small and more discrete incisions and do not run the risk of any contour or edge transition problems. There are no effective injectable methods of skull augmentation. While fat can be injected, its survival is highly unpredictable as well as how smooth it might be. (which it wouldn’t) But there are no adverse effect from using fat other than how well it may or may not work.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an extremely pronounced (Stage 4 I think) single glabellar line that was treated with Juvaderm and Botox multiple times back in 2007/2008. The single line is now gone but significant 11 lines that have formed around it. My current dermatologist has a concern with fillers and the glabellar region due to the blindness risk. Do you do Acellular Dermal Matrix Insertion? Is that a viable option? Is it an expensive procedure? What are my options for glabellar implants?
 A: I have placed about every conceivable graft material into glabellar lines. Acellular dermal matrix (ADM) is just one example and there are many other options including synthetic implants. The most common form of ADM would be Alloderm, which is an allogeneic cadaveric dermal product which has been around for years. It is placed in the office as a simple office procedure done under local anesthesia. But other implant types, such as synthetic Permalip implants can be used, which has a guaranteed volume retention. And are just as easily placed as any other glabellar graft or implant material.
A: I have placed about every conceivable graft material into glabellar lines. Acellular dermal matrix (ADM) is just one example and there are many other options including synthetic implants. The most common form of ADM would be Alloderm, which is an allogeneic cadaveric dermal product which has been around for years. It is placed in the office as a simple office procedure done under local anesthesia. But other implant types, such as synthetic Permalip implants can be used, which has a guaranteed volume retention. And are just as easily placed as any other glabellar graft or implant material.
While blindness is an extremely rare complication from the use of injectable fillers around the eyes, the way to completely negate that concern is a non-injectable implant placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I spoke to you all a while back about considering plastic surgery. I was very pleased with the results of the face prediction and your wonderful, fast replies. However, I have just a few questions:
1. How would I schedule an in person consultation? I would be coming from way across the country and I am willing to fly out to Indiana. The online Skype consultation will not really work because the internet is quite slow where I live and I am worried it’ll be more trouble than it’s worth. Therefore, I’d be more comfortable with an in-person consultation.
2. What is the estimated recovery time for Chin Reduction surgery and Rhinoplasty? Would I have to stay in Indiana for a certain amount of time? Are we talking days, or perhaps weeks?
3. I would be unconscious during the surgery, right? So, do you guys have a licensed anesthesiologist at all of your locations?
4. I see that you have multiple offices to choose from. Which office location would be the best for me and my procedure?
Thank you so much for taking the time to answer my question, and thank you all for your hard work.
A: In answer to your questions about rhinoplasty and chin reduction:
- An in person consultation can be arranged at your convenience. I will have my assistant Camille contact you next week to make those arrangements.
- The concept of recovery after any surgery can mean various things to different people. But to use a simple endpoint of being able to do most functions and looking only moderately swollen, think 10 to 14 days. You should be able to return home in a few days after surgery.
- Rhinoplasty and chin reduction surgery requires a general anesthetic to be both completely comfortable during surgery and to allow the best extent of the surgeries to be done.While I operate at multiple hospitals, aesthetic procedures are done at my private surgery center which is both AAAHC certified and staffed with board-certified anesthesiologists.
- At stated in #3 above, there is only one aesthetic surgery center at which I operate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 21 year old man and I was looking to have jaw angle implants with you. But first I would like to have your professional opinion if I really should get the implants? And to have better results should the implants be customized? And how much does it cost to have custom jaw angle implants?
A: In looking at the side view pictures that you have provided (which only provides an incomplete and one-dimensional view of the jawline), I see no benefit to jaw angle implants for you. You already have a fairly low mandibular plane angle (linear relationship of the jaw angle to chin line compared to the Frankfort horizontal line) and you would not want to drop it down any further. Whether there is any benefit to width only jaw angle implants requires a frontal view picture to make that assessment.
Jaw angle implants come in two fundamental types, width only and combined vertical and width angle types. The vast majority of patients, male or female, seeking jaw angle augmentation have a high jaw angle or a steep mandibular plane. This requires a vertical lengthening style. Less commonly, the angle position is vertically satisfactory and a more defined shape is needed through width enhancement
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As the date gets closer I’m just stressing a little. Just want to make sure the plan is clear. I just want to make sure you can make the tip smaller and more symmetrical. Not too pointy and won’t stick out too far. Nostrils smaller as well. I just want it to look pretty and feminine and still fit my face well. I know you are good at what you do and I trust you but just had to write you. Just need some reassurance. Thanks 🙂
A: Any patient considering any type of plastic surgery, particularly rhinoplasty which sits in the center of the face, will have presurgical anxiety. This anxiety stems from the uncertainty of what the outcome will be. This is why presurgical computer imaging is done, to help see if the general changes shown are what one is looking to achieve. Thus, it is fair to say that you will go through the surgery just fine and your nose will have an improved appearance afterwards as most of the imaging predictions shown will largely be achieved.
However, it is also important to understand that few rhinoplasties ever turn out ‘perfect’. There is always going to be some minor imperfections from the ideal desired result. It is also important to understand that the final results of a rhinoplasty take a long time to be realized due to the time needed for the overlying skin to shrink down to the reshaped bone and cartilage framework of the nose.
Point of this discussion is…your nose will look a lot more proportionate, it will still has some imperfections and one has to have patience in the recovery process.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am on a search to find the right doctor to fix my facial structure problem. I’ve been very dissatisfied with the worsening of this birth defect as I age and skin becomes more loose. I started to notice it when I was in my early teens but was very skinny at that time in my life. I am average weight and I tried just having chin liposuction which helped a little but is back to where it was and never really was even close to enough to fix my issue. It’s not only completely hinged crooked (bottom jaw bone) but I think the top of my skull is also off balance (which might not be a big deal in the end if not fixable with fillers/botox) I need professional analysis and advice. I don’t know how much bone I have on that side but i basically can only take photos on one side or it looks like i h ave a huge swollen tooth (I get asked, it kills my self esteem). I need to do this now. I can’t keep living my life with the constant reminder and pain that comes with it. Not if it’s something that I know can be fixed at least some. I also have an eye issue that will not be something that has to do with this surgery other than the fact that I think my entire face being on a tilt has caused strain on a muscle or nerve causing my limited vision on one side (luckily for me the way I can look straight with both eyes is also the side that I can pose to camouflage the extreme jaw imbalance). Please help! You have a lot of background knowledge and studies that go beyond most others I’ve seen. I need to know the long term problems etc. This is a risky and major surgery but is becoming more common. I was originally told locally that I would have to have my jaw broken, re-aligned, and all my teeth realigned as well which is not something I’m prepared to endure at 31years old. I’m looking for results that aren’t going to take years of adjustments and cost to fix while suffering through the pain. Let me know if you think you can help. Thank you!
A: What I see just in these two picture you have attached is a craniofacial asymmetry of which appears to be a hypertrophy problem on your left side. The first place to start is to make an accurate diagnosis and determine the extent of the facial bone differences between the two sides of your face. While there are a wide variety of facial procedures to help, careful analysis must first be done. This information can be obtained by getting a 3D craniofacial CT scan. This will allow both a visual and quantitative of your craniofacial asymmetry. With that information, treatment recommendations can then be made.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Love Band eyelid surgery and what to know how it is done. Am I a good candidate for this procedure?
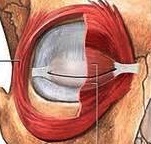 A: The so called Asian Love Band eyelid surgery (also called Youthlites) is conceptually double eyelid surgery for the lower eyelid. The objective of this procedure is to create a fullness below the lashline on the lower eyelid, representing an orbicularis muscle roll that naturally occurs in some eyelids. By so doing, it can make the to make the eye look larger and more open as it creates a lower eyelid that has two visible parts. This is an effect that is not unlike that created by the more well known Asian double eyelid surgery in the upper eyelids.
A: The so called Asian Love Band eyelid surgery (also called Youthlites) is conceptually double eyelid surgery for the lower eyelid. The objective of this procedure is to create a fullness below the lashline on the lower eyelid, representing an orbicularis muscle roll that naturally occurs in some eyelids. By so doing, it can make the to make the eye look larger and more open as it creates a lower eyelid that has two visible parts. This is an effect that is not unlike that created by the more well known Asian double eyelid surgery in the upper eyelids.
Some people do not have such a lower eyelid roll because their orbicularis muscle is thinner and more stretched. In my experience, I have seen Asians who naturally have an orbicularis muscle roll who want it removed. Conversely, I have seen other Asian patients who do not have it who want it created. (aka Love band lower eyelid procedure) Whether a skin roll under the lower eyelid lashline is viewed as aesthetically pleasing is a personal decision.
There are multiple ways to create the orbicularus roll effect and it is all about adding some form of a graft or implant to create that volume. A temporary Love Band effect can be created by synthetic injectable fillers as a non-surgical technique. Surgical methods include fat injections or the placement of a thin autogenous dermal, fascial or allogeneic dermal graft. (e.g., Alloderm) By adding volume on top of the orbicularis muscle, an outer visible roll is created. No matter what method is used for orbicularis muscle augmentation, recovery is fairly quick as it is just a limited version of a lower blepharoplasty incision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in knee lifts and want to know if I am a good candidate. Also have you done many?
A: Technically, a knee lift is a simple excisional procedure that is done for rolls of skin above the knees. It is a near full-thickness crescent of skin and fat removed along the suprapatellar crease. Because it is done directly where the skin rolls are, it is tremendously effective. But it does at the expense of a fine line scar above the knee in the crease so a prospective patients must be fairly motivated. (sees a fine line scar as a better alternative to the skin rolls) To keep the resultant scar as narrow as possible, it is important to preoperatively mark the amount of suprapatellar knee tissue excision with the leg both fully extended and bent at 90 degrees to prevent excessive excision of tissue and extreme tension on the scar
Knee lifts have very little recovery and are not associated with much discomfort. The only caveat is that one should avoid doing activities that risk bending the knee beyond 90 degrees for the first month after surgery.
Because of the scar concerns, the request for knee lifts is very infrequent, I have performed about a half dozen knee lift procedures in the past few years.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do you do or work with an OB/GYN who will do both the tummy tuck and partial hysterectomy during the same operation.
A: It has been historically common to do a hysterectomy and a tummy tuck at the same time for the obvious convenience of patient recovery and the access that a tummy tuck incision provides for the hysterectomy procedure. I have done it numerous times with various Ob-Gyn surgeons. That is still done today although not quite as commonly due to economic considerations. Now that hospitals are very conscious and diligent about collecting complete fees for the elective tummy tuck portion of the combined procedure (OR and anesthesia costs of which you will be responsible not your insurance) it becomes critical to look at the cost differences of having these procedures done together or separately. Depending upon the facility (hospital) the combined costs may be relatively minor compared to doing them separately or could be thousands of dollars more if done together in a hospital compared to having them staged apart. (tummy tuck done in a private facility)
Having good experience combining these procedures, we do know what that differential can be based on our own private plastic surgery center. I will have my office pass along that cost differential to you so you can see of such a combined procedure makes good economic sense for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in rhinoplasty but have one major question. My appearance changes greatly when I smile, my nose really flattens out and I would like it to be more defined when I smile. When my face is at rest, my appearance is satisfactory. My recent pics show no definition. Will rhinoplasty help solve this concern?
A: The concern about nostril flare with smiling is actually a fairly common question from patients considering rhinoplasty. It is important to realize that rhinoplasty is a static operation, not a dynamic one. It changes the nose structures based on their natural non-moving state. While it will give the nose more definition, particularly of the tip, it will not necessarily prevent the nostrils from flaring when you smile. That is a natural phenomenon of all noses as the facial muscles pull on the non-fixed bases of the side of the nostrils. While the nose will become more refined with the surgery, you should not expect that it will solve the flare of the nostrils that naturally occur from smiling. You should consider to undergo rhinoplasty for the changes you may see from computer imaging with your face at rest.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I see that you are able to narrow the width of the face by osteotomy of the zygomatic arch. In addition to this, I am concerned about the roundness of my cheeks, which have fairly prominent ‘apples’. I have fairly prominent cheekbones (I am of asian descent), so I was wondering if it would be possible to somehow reduce the body of the zygoma to reduce the prominence of cheeks when smiling? Or is it more of an issue to do with the amount of soft tissue? And if so, is there any way to reduce the fat in that area.
A: What you appear to be talking about is the soft tissue fullness of the cheek area rather than the bone. The term ‘apple cheeks’ almost always means an anterior cheek area that is not related to bone. This is an area that will not be affected by any bony repositioning. In some cases, small cannula cheek liposuction can be helpful in reducing this area of cheek fullness. It can be surprising sometimes how much fat can be extracted from the cheek and a few ccs can often be obtained. But it is not always successful and can be associated with some persistent after surgery swelling.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am average build. I was a patient a few years ago from a Groupon and received an estimate at that time. I had Smart lipo on my arms last spring, by a dermatologist, but the skin still bags below short sleeve tops, I would like to find out if there is anything that can help with that.
A: Unfortunately, getting liposuction through Groupon is probably not the best way to have any form of plastic surgery. By definition of the way Groupon works, you are going to get liposuction for the problem area (whether it would be effective or not) and are going to get the fastest and cheapest way to do it. It is not really any surprise that you have found the result wanting.
In looking at your pictures, without the benefit of not knowing what you looked like initially, I would say that any form of liposuction never had a reasonable chance to work. What you really needed all along is a formal arm lift. You have too much loose hanging arm skin to think that it could possibly be tightened by laser liposuction. You may not want the scar from an arm lift but that is the only treatment that is worth undergoing if you want a real arm shape change.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I previously had hydroxyapatite added along my jawline and my cheeks enhanced via zygomatic sandwich osteotomy. My jawline is somewhat asymmetric and some of the HA in the jaw area closer to my chin needs to be removed/remodeled. I would also like my cheeks enhanced via HA as the augmentation is not adequate and also somewhat asymmetric.
I am not sure if you are familiar with all of these procedures and realize this is not a straightforward case. Essentially I would like the the jaw area remodelled for better symmetry by removing HA and the cheeks enhanced further by adding HA.
I am not sure if you use HA, from reading your website it sounds like you don’t however your opinion as a long standing plastic surgeon would be invaluable to me. I am also not opposed to any ideas you might have or getting the jaw remodelling done by yourself.
Thank you very much for your time and consideration.
 A: Thank you for telling your story and sending your pictures. I am very familiar with using hydroxyapatite (HA) block and granules as back in the 1980os and early 1990s that was the way much of facial augmentation was done. I still do it occasionally on patient request. HA has fallen out of favor for many surgeons as the blocks are hard to shape and stabilize and the granules are somewhat unpredictable in shape with healing.
A: Thank you for telling your story and sending your pictures. I am very familiar with using hydroxyapatite (HA) block and granules as back in the 1980os and early 1990s that was the way much of facial augmentation was done. I still do it occasionally on patient request. HA has fallen out of favor for many surgeons as the blocks are hard to shape and stabilize and the granules are somewhat unpredictable in shape with healing.
I suspect you had HA blocks put in with your zygomatic osteotomies which is good for width but not so much for projection. HA granule ‘sandwiches’ can be made which helps control the material to some degree for secondary placement on the cheeks for greater projection.
Removal of the HA along the jawline is tedious but doable since it was likely injected intraorally along the jawline.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in having an abdominoplasty performed. But a a little history…I was overweight my entire childhood, finally reaching 320 lbs by late 2011. I made some big changes and lost most of the weight very quickly, about 90 pounds in the first year. I have been hovering around 190 lbs for over a year now and am generally happy with my weight. I have completely changed my diet and know I will never go back to my old ways. The only evidence of my former self resides in my chest, stomach, and inner thighs. There is some loose skin on my upper arms as well, but I’m not too concerned with that. I’ve attached some pictures to get your opinion. What kind of procedure do you think would be best for me?
A: From an abdominal standpoint, the roll of excess skin goes all around the waistline so a tummy tuck must be a near circumferential technique to really get all the excess skin out. Male tummy tucks are unique because they never require muscle tightening since there is no rectus diastasis from prior pregnancies. So it is essentially getting out all the loose skin and that probably encompasses at least a ‘300 degree’ excision length. The chest is always the most challenging in any male weight loss patient due to the skin and nipple sag and the inability to tolerate the scar locations from traditional breast lifting procedures that women undergo. (since they are being left with a breast mound while men want the chest flat) In my experience, all such chest reshaping procedures in many male weight loss patients leave me wanting for better results than they often produce, but the key is to not have any procedure that leaves with the trade-off of unsightly scars. In your case, I would recommend a periareolar reduction technique with liposuction. Whether any more than that would be indicated would require a true frontal picture so I can better assess what degree of chest sagging you have. (your current chest picture is taken from below and that may make it look less saggy that it really is)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I am a young African American woman. I have a larger forehead which I can live with. The problem I have is that since my forehead is wide and protrudes and my nose is stubby, it makes my glabella look flat and too wide. I would like a glabella that makes my face look more define. What do you suggest? Thank you.
A: Thank you for your inquiry and sending your pictures. What you really have is a combined glabellar (forehead) and nasal bridge ‘defect’ or recessed area. This glabellar-nasal area lacks the protrusion and dimensions that the rest of your face has so it is disproportionate. (or as you have accurately stated…too flat) Building up this area could be done in multiple ways. The simplest would be fat injections but that carries with it the unpredictability of how well the fat would survive. The best approach is to really have a custom glabellar-nasal bridge implant made as a single piece. A standard preformed nasal implant will not augment the globular region of the forehead. Such a custom nasal implant would be placed through an open rhinoplasty approach (low) with an endoscopic technique from above. Other strategies include a preformed nasal bridge implant combined with bone cement augmentation of the glabella. As you can see there are various augmentative strategies using different materials.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know what can and cannot be done about untreated plagiocephaly in terms of facial asymmetry surgery procedures. I am still young (19), which is why I want to explore my options now so I can put this ongoing struggle in the past. I have very noticeable facial assymetry, particularly evident in my cheeks and jaw angle. I also have some forehead assymetry as well due to the soft spot on the left back side if my head. Regardless of this, the area of immediate concern is my cheeks and jaw. The left side of my face is much more prominent and “fuller” due to the Plagiocephaly. My eyes are also assymetrical because of the different orbital positions making it seem as if I have a lazy eye when looking in certain directions. Another area of concern for me is my flat midface; it seems as if I need at method to someho w “pull out my face.” My face needs to gain a more 3D look so my eyes don’t seem deeper than they actually are. Also, as you can tell from the pictures, not only do both halves of my face look drastically different from the side, my head lacks length from the front of my head to the back, as well. I would like to gain your input on what would be the most effective methods to improve my facial features.
A: What you are describing are very typical facial findings from congenital occipital plagiocephaly. While there is a long list of facial and skull changes that can be done for our facial asymmetry surgery, the question is which ones have the greatest value and are the most economically efficient. You have pointed out the most important to you currently and that is the flatter and more deficient cheek and jaw angle on the affected side. A cheek and jaw angle implant will help in that regard. But it is important to point out that the eye on the same side is also a major focal point and addressing it with orbital floor augmentation and a corner of the eye adjustment would also be important. ideally the best way to treat all three facial skeletal issues would be a 3D CT scan to make the implants match the facial structures on the opposite side the best.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a woman with square jaw who just wants to have her angles rounded off, nothing extreme…so far, the people I’ve seen who have had jaw angle reduction/resection were left with no angles at all and I found it unnatural and unattractive. I saw a professor who talked to me about bone decortication, removing a little bit the angles without touching the bone or touching the muscle and that it can be done under local anesthesia with little risks and would give a natural result. But he said that asymmetries are common with that type of method. Is that all correct?
A: Jaw angle reduction/recontouring can be done by two basic methods, bicortical (amputation) or monocortical. (decortication) While the historic and still most commonly used technique is bicortical removal, you are correct in that such amount of bone removal can make the jaw angle ‘hollow’ and create a soft tissue sag or indentation over the jaw angles. For many patients, a monocortical approach may be better as it lessens jaw angle width but without losing jaw angle shape. The best candidates for this type of jaw angle reduction surgery are those that have radiographic comfirmation of an angle flare that sticks out beyond the external oblique ridge of the mandibular ramus. This makes it technically possible to reduce the jaw angle flare with the instruments that are available to do it.
But no jaw angle recontouring method can really be effectively done under local anesthesia. (nor can I imagine who would want to) It is necessary to lift the masseter muscle off the bone to provide visualization for the bone reduction. Any method of jaw angle manipulation (augmentation or reduction) run the risk of asymmetry because they can not be seen as a ‘pair’ surgically and most people do not have perfect jaw angle symmetry beforehand.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a silicone forehead implant placed through a scalp incision after an injury which left an indented forehead. I still have a high hairline so I want to do hair grafts or transplant. My question is can they still put hair transplants over silicone implant or will the hair not stay and grow? The implant goes from my brow bone all the way to middle of scalp.
A: The location of any skull implant, like a forehead implant, is way down at the bone level. This is numerous tissue layers away from where the hair follicles are located which are just under the skin. Thus any forehead or skull implant will not have any negative impact on hair transplants anymore than the overlying existing hair that is there now. You can freely have hair transplants done along the frontal hairline without fear that they will not take and subsequently grow. I have had numerous patients have this done, including women, with very successful hair transplant results.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 40 year old female in good health and I have a 7mm epidermoid cyst on my forehead, just above my right eyebrow. I had an ultrasound scan which shows that it is quite deep near the skull. The report states that it is a benign looking 7mm cyst which looks subgaleal and is located in the region of the right glabella. However it is having an effect on my self-esteem and I would like to know what options I have for removal and whether a direct excision would be the best and safest option or to if it is worth getting it removed by endoscopic surgery?
In particular I am worried about what the scar will be like if I get it removed directly since I am of Asian origin and am I am concerned about the scarring. I am exploring whether having it removed endoscopically would be worth-while given my concerns over scarring.
Because my cyst is located further down near the eyebrow would this be more of a risk and more difficult to remove by endoscopic surgery? By doing an endoscopic surgery would this cause an indent or depression where the cyst was removed?
Would the benefits outweigh the risks and would there be any risks of a depression at the location after the endoscopic removal?
I would be interested in hearing your views about this and whether this is an option worth exploring. I would greatly appreciate your feedback.
A: Dermoid cysts are exceedingly common around the eye area and are often located down at the bone level. In many cases, they will even leave a little depression in the bone. While an endoscopic approach would be preferable from a scar standpoint, the question is whether this approach can technically be done given how low it is on the forehead. I can not really comment on this technical aspect without seeing a picture of where it is on the glabella region. Most likely it can be removed endoscopically having done it this way myself numerous times.
Whether its removal will leave a depression can not be predicted. But given its relatively small size, I suspect it may not. But you can always hedge that bet by placing a small fat graft in its place at the same time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I went to Asia and had mandible angle jaw reduction. Now my face looks deformed with a protruding bulging area as well as indented area on my jaw line. Please can you have a look at my attached images. I now have CT scans. Please let me know what you think has happened. I need help and just don’t understand what has happened. The surgeon in Asia was suppose to only cut the posterior jaw angles off to get rid of the square jaws. However, something has gone wrong and I really need help. Please see my CT scans, I would really appreciate you giving me an idea of what might have happened. (I may need some kind of jaw implants for a corrective surgery. However, it is alright with me if you are not happy to give me a corrective surgery as I understand most doctors don’t like doing corrective surgeries. ) I’m trying to find out what might have happened from my previous surgery /jaw angle reduction, and I don’t understand the CT scan. ) I would appreciate any help as I really need help.
A: What happened to your jawline is very simple. They cut off the angles completely. The bump you see on the jawline is the front end of the cut where it is not smooth with the rest of the jawline. The indented area is the loss of bone support for the soft tissues from the removal of the jaw angles. You are a classic example of why the jaw angle reduction with an amputation technique is usually not a good operation. It would be better to have a lateral shave of the jaw angles so the bony support is not completely lost. Restoration will require some form of a jaw angle implant that provides vertical length but no width.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to make a few enquiries regarding facial implants.
My plan is to have bespoke implants fitted precisely over my current facial skeletal bone structure to adjust the appearance. I am interested in various different locations on the face, and I know fairly precisely the dimensions of the facial appearance I would like to have. I was wondering if you have an information pack for new patients for this procedure and some advice on getting started?
My second questions is in regards to the materials used for the implants. On your website, you mention two materials – silicone and Medpor. I was wondering if you ever work with, or would consider working with 3D printed titanium implants. the reason I am particularly interested in this material is the strength advantage it has over others.
A: The best way to get started is to send me some pictures of your face and a detailed list of what you want to achieve and where you envision the augmentations to be done. Using that information, custom implant designs can be done on a 3D CT scan which you would need to get. That CT scan can be done in your local community.
As for custom facial implant materials, only silicone is currently available for use as a custom facial implant material for 3D CT fabrication. While I am certainly not opposed to using any other material, such as titanium, you have to factor in other important considerations such as cost and access. Very stiff materials, such as titanium, require much larger incisions to place dependent on their size and location. This is an issue that patients never think about but can be a very limiting issue. In addition, there is no advantage to a stiff metallic material as an implant. Since bone is the backing for all implant materials, they all become firm and ‘bone-like- once in place.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a very burning question about calf augmentation by fat injection .I know my appointment is coming up soon on the 22nd but the closer it gets, the more anxious I am. I know not to have too much expectations but is there a away to enhance the outcome, for example, do you add anything to the fat to make them more viable?And is there anything I can do to improve the results?I totally think my calves are the skinniest anyone can ever imagine and so will I really have enough fat to make them as bigger as possible? If I will need a touch up, do I have to go through the entire procedure or do you preserve some fat from the first procedure. Thanks.
A: The methods to enhance fat injection graft take are how the fat is concentrated at the time of its harvest prior to its injection. Some enhancement of fat graft survival has been noted from adding PRP (platelet-rich plasma, a blood extract) but that evidence is not conclusive. Since it is your own blood extract it is perfectly safe. But whether it truly improves fat graft take is not clear.
Harvested fat can not be preserved for a secondary or touch-up procedure. It is technically possible to do so but it has been shown that none of that frozen fat will survive when injected later.
Dr. Barry Eppley
Indianapolis, Indiana