Shoulder Reshaping Surgery/ Clavicle Shortening/ Shoulder Lengthening
Shoulder Reduction & Widening Surgery
SHOULDER FEMINIZATION
 The desire for more narrow shoulders is for those patients who seek a more feminized appearance to their upper torso. This is typically requested in the transgender male to female or the cis-female patient. In my experience such requests are equally split between these two patient groups. Shoulder feminization is achieved by removing a segment of bone from the clavicles which allows the bideltoid distance to decrease. This occurs because anatomically the clavicle is the lone horizontal bone of the body and the only structure that keeps the shoulders away from the sternum.
The desire for more narrow shoulders is for those patients who seek a more feminized appearance to their upper torso. This is typically requested in the transgender male to female or the cis-female patient. In my experience such requests are equally split between these two patient groups. Shoulder feminization is achieved by removing a segment of bone from the clavicles which allows the bideltoid distance to decrease. This occurs because anatomically the clavicle is the lone horizontal bone of the body and the only structure that keeps the shoulders away from the sternum.

 While removal of a segment of the clavicle is a straightforward concept, adapting it for an aesthetic operation with acceptable scarring and low risks requires numerous surgical technique modifications from traditional clavicle surgery used in the treatment of fractures. Where to place the incision, how much bone to remove and the method to hold the shortened clavicle in place as it heals are the three important steps in aesthetic shoulder width reduction surgery.
While removal of a segment of the clavicle is a straightforward concept, adapting it for an aesthetic operation with acceptable scarring and low risks requires numerous surgical technique modifications from traditional clavicle surgery used in the treatment of fractures. Where to place the incision, how much bone to remove and the method to hold the shortened clavicle in place as it heals are the three important steps in aesthetic shoulder width reduction surgery.


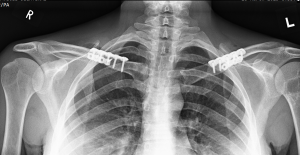
 The placement of the incision is directly above the best location to remove the segment of clavicle bone which is at its inner third. This is the thickest part of the clavicle by cross-sectional diameter and is also the most stable being closest to the sternum. The small skin incision is placed, not over the bone, but up above in the supraclavicular fossa which provides for the most favorable scar healing. The segment of bone removed is typically in the range of 2.0 to 3cms per side. Short rigid plate and screw fixation of the shortened clavicle is used for stabilizing the two bone ends. This results in a bideltoid width reduction of 5 to 6 cms which creates a a more narrow and slightly rounded shoulder appearance. This has also been shown to result in uncomplicated bone healing and no adverse effects on shoulder function.
The placement of the incision is directly above the best location to remove the segment of clavicle bone which is at its inner third. This is the thickest part of the clavicle by cross-sectional diameter and is also the most stable being closest to the sternum. The small skin incision is placed, not over the bone, but up above in the supraclavicular fossa which provides for the most favorable scar healing. The segment of bone removed is typically in the range of 2.0 to 3cms per side. Short rigid plate and screw fixation of the shortened clavicle is used for stabilizing the two bone ends. This results in a bideltoid width reduction of 5 to 6 cms which creates a a more narrow and slightly rounded shoulder appearance. This has also been shown to result in uncomplicated bone healing and no adverse effects on shoulder function.
 One of the most common questions about shoulder reduction surgery is in the amount of bone that can be removed and what effect it creates. The visible change in shoulder width occurs as a result of both horizontal bone length reduction as well as some forward rotation of the shoulders. The rounding effect of the shoulders comes from the anterior rotation which appears to be relatively minor as it relates to perceived width reduction.The typical amount of clavicle bone removed is between 2 to 3 cms based on patient body size and natural shoulder width.The question of how much bone can be safely removed is based on its effect on bone healing and postoperative shoulder function. Extrapolating from the orthopedic surgery experience in clavicle fractures, bone shortening in the 2.5cm+ range is not associated with abnormal scapulohumeral kinematics. This indicates that no negative shoulder functions should occur in elective clavicle length reductions in the range of 2 to 3cms. What would happen beyond 3cms to 3.5cms of clavicle length loss in a bilateral procedure has unknown effects for shoulder function.
One of the most common questions about shoulder reduction surgery is in the amount of bone that can be removed and what effect it creates. The visible change in shoulder width occurs as a result of both horizontal bone length reduction as well as some forward rotation of the shoulders. The rounding effect of the shoulders comes from the anterior rotation which appears to be relatively minor as it relates to perceived width reduction.The typical amount of clavicle bone removed is between 2 to 3 cms based on patient body size and natural shoulder width.The question of how much bone can be safely removed is based on its effect on bone healing and postoperative shoulder function. Extrapolating from the orthopedic surgery experience in clavicle fractures, bone shortening in the 2.5cm+ range is not associated with abnormal scapulohumeral kinematics. This indicates that no negative shoulder functions should occur in elective clavicle length reductions in the range of 2 to 3cms. What would happen beyond 3cms to 3.5cms of clavicle length loss in a bilateral procedure has unknown effects for shoulder function.







































































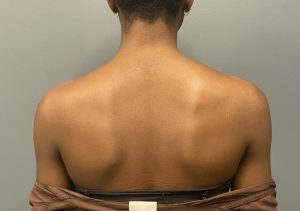
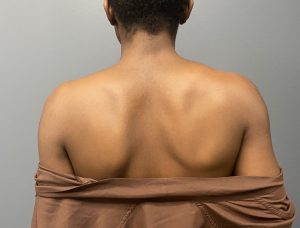























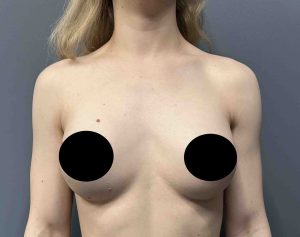
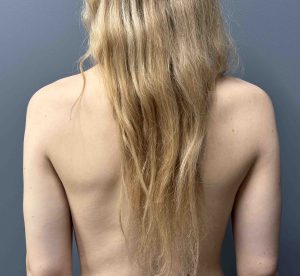
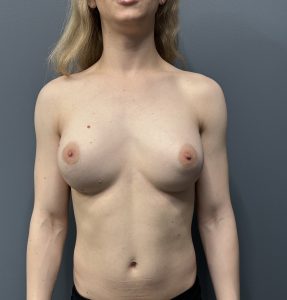
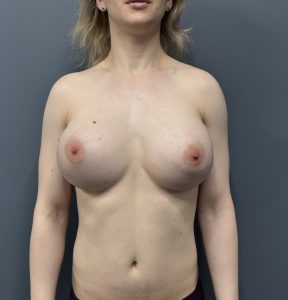
One year postop


















Combining breast augmentation (425cc silicone implants) with shoulder narrowing surgery.











![]()
![]()
![]()
![]()
![]()














































































While most patients have both shoulders narrowed at the same time (bilateral clavicle reduction osteotomies), a few patients may prefer to separate the procedure into two stages. While lacking the efficiency of a bilateral procedure, a staged approach does offer a less challenging recovery (with one good arm) and can be performed as an outpatient surgery. The timing between the two stages is patient dependent but having full arm range of motion on the first shoulder narrowing makes sense before proceeding with the second surgery. (minimum of 6 to 8 weeks)











While the vast majority of shoulder narrowing patients are transgender there are some cis-females that undergo the procedure as well. There is no difference in the surgery between the these two patient populations. There may be some slightly different motivations for the surgery but the Intraoperative technique and outcomes are identical.



The aesthetic outcomes in shoulder width reduction surgery is fundamentally about how much width reduction is visually achieved and how well do the supraclavicular scars look long term. As would be suggested by the amount of clavicle bone removed it is a near 1:1 relationship so most patients can expected an approximate 1 inch reduction per each shoulder. But shoulder narrowing is more than just about how much numerical reduction in shoulder with that is achieved. An equally important effect is the more rounded (less square ) shape to the shoulders that results.
Shoulder Asymmetry



While differences in the length of the clavicle is normal (usually the left clavicle is a bit longer than the right) it usually is either not noticeable or bothersome to the patient. But when it is some adjustment in the amount of bone removed on the longer side can be done. This can provide some reduction in the asymmetry but unlikely to make it perfectly symmetric.
Aesthetic Outcomes
 Aesthetic outcomes in shoulder width reduction surgery is fundamentally about how much width reduction is visually achieved and how well do the supraclavicular scars look long term. As would be suggested by the amount of clavicle bone removed it is a near 1:1 relationship (close to 0.9) so most patients can expected an approximate 1 inch reduction per each shoulder. But shoulder narrowing is more than just about how much numerical reduction in shoulder with that is achieved. An equally important effect is the more rounded (less square ) shape to the shoulders that results. Most supraclavicular scars do well as defined by how many patients have ever requested a scar revision for them…which is very low in number.
Aesthetic outcomes in shoulder width reduction surgery is fundamentally about how much width reduction is visually achieved and how well do the supraclavicular scars look long term. As would be suggested by the amount of clavicle bone removed it is a near 1:1 relationship (close to 0.9) so most patients can expected an approximate 1 inch reduction per each shoulder. But shoulder narrowing is more than just about how much numerical reduction in shoulder with that is achieved. An equally important effect is the more rounded (less square ) shape to the shoulders that results. Most supraclavicular scars do well as defined by how many patients have ever requested a scar revision for them…which is very low in number.
Recovery
Recovery from shoulder width reduction surgery is unique and should be differentiated from clavicle fracture repair. Because it has no associated soft tissue trauma like which occurs in clavicle fractures and is a very isolated procedure to just one small section of the bone, it is associated with less discomfort after surgery. However because it involves two shoulders (unlike clavicle fractures) it has some greater early functional limitations. Arm motion is restricted to the first few weeks after surgery to keeping the elbows close to the body. Thereafter a gradual progression of range of arm motion is done until 6 weeks after surgery when raising the arms above one’s shoulders can be permitted. Any strenuous physical activities should not be done until two to three months after the surgery.
Clavicle Hardware Removal


A common postoperative question is whether the plate and screw hardware will ever need to be removed. Usually it does not unless it causes symptoms such as discomfort or visibility. The latter is the most common reason for removal which can be done anytime after 12 months or one year from the original surgery. Hardware removal is not associated with the significant recovery associated with the initial clavicle reduction surgery in terms of arm range of motion restriction.
Combination Shoulder Reduction Surgeries
A common question with shoulder reduction surgery is whether it can be conbined with other body or facial contouring surgeries. The answer to that question lies lies in the patient’s recovery in the patient’s recovery and not the ability to have the combination surgery performed. In the operating room almost any number of procedures can be performed but careful consideration must be given to how that influences the patient’s recovery. Given that the primary recovery issue in shoulder reduction surgery is the use of one’s arms one has to consider how other procedures may influence the recovery process. As a result it is easy to see that procedures such as primary or secondary breast implant surgery, for example, or any form of facial surgery will not have a significant adverse effect on the recovery process in terms of severity or duration. Conversely more significant body contouring surgeries like rib removal or buttock and hip implants may. As a result careful consideration needs to be given in patients with these combination surgeries to ensure that they have adequate postoperative support as well as being properly prepared for the recovery process.
 .
.


SHOULDER MASCULINIZATION
 Widening of the shoulders in a male can be done by several different surgical techniques direct or indirect. Unlike shoulder narrowing, in which there is only one way possible to do so, shoulder widening has three options which are performed at two very different tissue locations. The direct approach is augmentation of the shoulder muscles. Deltoid implants can be placed at the subfascial or submuscuar locations or fat injections can be done into the muscle and subcutaneous tissues The indirect approach is to increase the bony length of the clavicles.
Widening of the shoulders in a male can be done by several different surgical techniques direct or indirect. Unlike shoulder narrowing, in which there is only one way possible to do so, shoulder widening has three options which are performed at two very different tissue locations. The direct approach is augmentation of the shoulder muscles. Deltoid implants can be placed at the subfascial or submuscuar locations or fat injections can be done into the muscle and subcutaneous tissues The indirect approach is to increase the bony length of the clavicles.
 Each shoulder augmentation method has their own advantages and disadvantages. Muscle augmentation by either fat injection or the placement of subfascial deltoid implants provides a direct augmentation effect whose width increase depends on how much fat survives or the thickness of the implant. These two shoulder augmentation methods provide a fairly limited recovery period but have the known associated disadvantages of implant-related risks and the unpredictability of fat graft survival.
Each shoulder augmentation method has their own advantages and disadvantages. Muscle augmentation by either fat injection or the placement of subfascial deltoid implants provides a direct augmentation effect whose width increase depends on how much fat survives or the thickness of the implant. These two shoulder augmentation methods provide a fairly limited recovery period but have the known associated disadvantages of implant-related risks and the unpredictability of fat graft survival.



 As the clavicles can be shortened for shoulder narrowing they can also be expanded or lengthened by a similar osteotomy location. A sagittal split osteotomy can be done at the mid-shaft of the clavicle which allows the bone to be lengthened while a central full-thickness contact of the bone is maintained. In this method partial thickness horizontal back cuts are made in the bone connected by a full-thickness vertical or sagittal cut between them. The outer clavicle segment is then slide out to the desired amount of lengthening, or the amount of lengthening the shoulder tissues will permit to occur, and the two overlapping central segments screwed together. A long superior clavicle plate is then applied with three screws on each uncut full thickness clavicle segment. The partial thickness bone gaps are filled in by the application of tissue back precision cut fibular bone grafts.
As the clavicles can be shortened for shoulder narrowing they can also be expanded or lengthened by a similar osteotomy location. A sagittal split osteotomy can be done at the mid-shaft of the clavicle which allows the bone to be lengthened while a central full-thickness contact of the bone is maintained. In this method partial thickness horizontal back cuts are made in the bone connected by a full-thickness vertical or sagittal cut between them. The outer clavicle segment is then slide out to the desired amount of lengthening, or the amount of lengthening the shoulder tissues will permit to occur, and the two overlapping central segments screwed together. A long superior clavicle plate is then applied with three screws on each uncut full thickness clavicle segment. The partial thickness bone gaps are filled in by the application of tissue back precision cut fibular bone grafts.

 The sagittal split osteotomy method should provide good healing of the central full thickness overlapping bone segments provided the plate and screw fixation remains stable. In the partial thickness defects created by the lengthened sagittal split of the bone healing is promoted by the use of solid bone grafts. I find now that this is superior to the previous use of bone putty.
The sagittal split osteotomy method should provide good healing of the central full thickness overlapping bone segments provided the plate and screw fixation remains stable. In the partial thickness defects created by the lengthened sagittal split of the bone healing is promoted by the use of solid bone grafts. I find now that this is superior to the previous use of bone putty.
The limits of the amount of clavicle lengthening that can be achieved is controlled by two factors, the geometry of the sagittal bone cut but, more importantly, the restrictions of the shoulder tissues to be pushed outward. The soft tissue attachments to the humerus and scapula have a blocking effect on the shoulder joint moving laterally. Most patients should be able to achieve 15mms per side with the maximum amount being 20mms per side. (the limits of the ability of the superior plate application which must be done outside of the split bone area)



 Clavicle lengthening osteotomies are obviously more invasive and have a much longer recovery period than any of the other two outer shoulder augmentation methods. But they offer an autologous shoulder augmentation effect as lengthening the natural shape of the clavicles creates both a widening and slight pull back look to the shoulders. This approach also may have appeal for those men who seek the ultimate natural approach to achieve shoulder augmentation even if one can probably not achieve as much of a shoulder widening effect as they would desire.
Clavicle lengthening osteotomies are obviously more invasive and have a much longer recovery period than any of the other two outer shoulder augmentation methods. But they offer an autologous shoulder augmentation effect as lengthening the natural shape of the clavicles creates both a widening and slight pull back look to the shoulders. This approach also may have appeal for those men who seek the ultimate natural approach to achieve shoulder augmentation even if one can probably not achieve as much of a shoulder widening effect as they would desire.



A detailed description and pictures of your concerns allow for the most informed response.
Disclaimer: By submitting a question, you agree that it may be used for educational purposes. Any identifying details or photos will be removed. Responses are general and not a substitute for medical advice.
North Meridian Medical Building
Address:
12188-A North Meridian St.
Suite 310
Carmel, IN 46032
Contact Us:
Phone: (317) 706-4444
WhatsApp: (317) 941-8237