Your Questions
Your Questions
Q: Dr. Eppley, I understand Dr. Eppley has performed dermal fat injections to treat coccydynia. I recently had this procedure done and for about 4 weeks it completely eliminated my tailbone pain. But the pain returned not long afterwards and now my pain is the same as it was before surgery. My plastic surgeon is attempting the surgery again in a few weeks. My question is, does Dr. Eppley have a list of post op recommendations to increase the success of dermal fat injections? I was told I can exercise fully after 4 weeks, including using weights and I wonder if that was detrimental to the surgery.
A:I don’t do fat injections for coccydynia and have never have for the very reason you have experienced….100% of the injected fat will resorb and the benefits will be very temporary (4 to 6 weeks). I do dermal-fat grafts not injections. This is the placement of a solid fat graft through an open incision with or without some tailbone bony reduction. This type of solid fat graft has a much higher incidence of survival and is far superior is pressure area lie the coccyx.
FYI Fat injections (liquid) is not the same as a solid fat graft.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,Is subcostal rib margin shaving/reduction completely put of question for a kidney pancreas transplant patient who is 5 years in and has never had an episode of rejection? I imagine rib remodeling is because the patient needs to wear a corset for months which i would think probably puts pressure on the transplanted organs.
A:Your supposition about not doing rib reduction in the kidney-pancreas transplant patients is correct. This would not be a good benefit to risk ratio.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am contacting you now because I have come across your case report about correction of sagging buttocks: https://exploreplasticsurgery.com/plastic-surgery-case-study-long-term-persistence-of-the-infragluteal-fold-in-lower-buttock-lifts/
I have one patient with a double fold after liposuction in the dorsal thigh area about 18 months ago. She has tried thread lift, fillers and some skin tightening at other clinics with no result. We have been discussion a surgical procedure similar to what you have described in your case report.
In my experience it is always difficult to elevate tissues against gravity long-term, and I have told her that there is a risk that the native gluteal fold with time will appear lowered even though if we can correct the double fold. However, you seem to have overcome this; your results are not only nice but also are long-lasting.
Therefore, I wonder if you could elaborate a bit on which sutures that you use (permanent?), and if there are any other pearls/caveats that could be useful to know.
A:One of the most common reasons for lower buttock lift surgery is when liposuction is done for the banana roll deformity. Having done many lower buttock lift surgeries I have never found descent of the re-created fold to be a problem.. Technically the excision creates the elevation of the fold and efforts to deliberately lift the fold are not really needed. By definition it is the overhang that is being removed and the excision merely re-establishes the original fold which was not visible because of the overhang. This is what you see when liposuction suction has created the problem which is really a form of pseudo ptosis. Why all of the other trial procedures do not work is because they simply cannot get rid of what is a tissue excess. That concept of a lift through threadlifts and skin tightening is an erroneous concept for the problem. You can’t lift or skin tighten away tissue excess
With the excision I secure the dermal edges of the excision down to the gluteal fascia. I don’t use permanent sutures, rather In use long lasting resorbable sutures.
The biggest postoperative problem i lower body lifts, as defined by the need for revision on surgery, is not the descent of the fold but some hypertrophic scarring which may require a secondary scar revision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I am wondering what can be done regarding a protrusion at the top of my head where I believe the coronal sutures come together(?!).the protrusion is like a line that goes from left to right, not front to back. It is a pronounced raised line that I worry about for aesthetic reasons.
A:You are likely referring to a raised coronal suture line which can cause a transverse protrusion. If the bone is thick enough it can be reduced by burring. A preoperative CT scan is done to make that determination.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to make jawline/chin/bone implants for the face permanent? By permanent I am talking about the implant fusing over time and becoming bone. It bothers me that if I have a silicone implant if I hit my jaw hard on something by accident or get punched it may slightly change position.
A:No type of implant material currently used for jaw implants can ever turn into bone over time. In fact no current implant material even has the ability for bone to bond to its undersurface where it contacts the bone. Fortunately those issues are actually irrelevant when it comes to any postoperative concerns about any type of implant material moving with trauma later. Between the early benefits of screw fixation and the more important encapsulation process that happens with scar tissue forming around the implant within the first six weeks of surgery it is impossible for the implant to ever move later. This is well known to surgeons who perform this type of surgery when they have to secondarily reposition or replace an existing implant. The encapsulating scar makes that procedure challenging. It is also important to recognize that most custom jaw implants have large surface area involvement which results and a lot of encapsulating scar over and around the entire implant. Of all the potential issues that one could have about jaw implants long term movement due to trauma is simply not one of them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a BBL with buttock implant five years ago. My buttock Implant are malpositioned, flipped and sagging and they split out of the muscle. What can be done now?
A:Thank you for sending your pictures. Based upon your description of concerns your buttock implants would have to be outside of the muscle as this would be the only reason they would flip and/or sag. Intramuscular placement about it implants is not associated with implant flipping or sagging.
I obviously have no information as to what the specifics of your buttock implant surgery as to how they were initially placed. It would be most helpful, if possible, to see the operative note from your surgeon from that surgery.
That being said, knowing that they were 455cc implants, in my experience those would be very difficult to get complete muscular coverage even if they tried to place them on an intra-muscular basis. Even if they got complete muscular coverage over them the size of implants would ultimately split the muscular closure due to pressure and they would have ended up either completely or partially outside of the muscle. Once outside the muscle then they can flip and sag. It would be easy to confirm this diagnosis with a CT scan if there is any doubt about the current implant location. However, a physical exam would likely provide verification of my explanation.
To solve this problem implants would need to be repositioned into the intramuscular space. It would be prudent to downsize the implants to the 350 to 400 mL range to successfully do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I underwent aggressive liposuction on my legs, which resulted in skin laxity and uneven skin surface, with dimples, protrusions, and irregularities. I am looking for an experienced surgeon in calf augmentation who can properly assess my case and give me the best recommendation.
A:Thank you for your inquiry and sending your pictures. I believe your fundamental question is whether calf implants will improve your skin laxity and uneven surface contour. The answer is that it will not. Calf implants are placed on top of the muscle under the fascia which also only goes about halfway down between the knee and the ankle. While it will make the appearance of the calfs bigger I would not count on it improving the problems that you have which are at the subcutaneous tissue level… a tissue level that is above that of the muscle. Calf implants will probably make a little bit of improvement in these issues but my point is that if you’re expecting a major or a complete eradication of all of the contour problems that have been created by the liposuction then you will be disappointed. One undergoes implants for the primary goal of bigger calfs. If any improvement in the skin contour is obtained that would be considered a bonus but not an expected outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Why is barred chest surgery in such a gray zone? It seems like surgeons are completely belittling it and not even trying to do anything about it.
A:Barrel chest surgery is not in the gray zone. It literally is in a no zone as it has never been performed before and understandably it has increased risk and unknowing benefits of performing the procedure. Only now is lower rib surgery becoming more mainstream but anything above rib 10 is completely unknown to any surgeons except the very few who have ever done it…. which to my knowledge is only me. The question is not whether it can be done whether would it be worth the surgical effort and potential risk to do so for primarily an aesthetic concern. Another words how much benefit can actually be obtained given the effort involved. Until one day the procedure is actually done on a patient those answers will remain unknown. But you can’t fault surgeons for not willing to take on those risks when the benefit is not known.
I think the fundamental problem with barrel chest surgery is to obtain a good improvement you have to treat all of the ribs probably from #4 down to #9 on both sides. That would be quite a surgical undertaking as well as the risks of pneumothorax x 10. That might be I’m to consider if we knew the good benefits could be obtained. But given that we don’t you can see the great hesitancy to do so.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
 Q: Dr. Eppley, Hello i had a forehead augmentation done with dr eppley and planning to get a temporal lift i just want to ask if this is risky as i have an implant on my forehead.
Q: Dr. Eppley, Hello i had a forehead augmentation done with dr eppley and planning to get a temporal lift i just want to ask if this is risky as i have an implant on my forehead.
A:One can safely have a temporal lift with an underlying forehead implant. The implant in these situations can actually be beneficial as it allows for convenient suture anchorage that is easier to place that doing it through the bone or temporal fascia.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, A few questions: 1. In your experience, is it very possible, by means of the various procedures you offer, to go from a non-model to a model-look, as defined by the actual beauty-standards of today? If so, what procedures are often required for this? 2. To achieve the Hunter eye look, one of the essentials is upper eyelid hooding. In your experience, is an infraBROW-implant better than fat grafting in the area? Can both be combined? Is one usually enough? 3. Can the fat harvested through say perioral liposuction be used as an injection in the upper eyelid or nasolabial folds in the same surgery? Thank you.
A:In answer to your questions:
1) What you are referring to when asking about going for a non-model to a model look is whether you can take an average looking male and make them look like a male model. In general, except for the rarest of circumstances, this is not an achievable outcome.
2) to achieve upper eyelid putting the most effective approach for most patients is going to be fat grafting. Whether it is best to do a combined brow bone in implant with the fat grafting must be determined on an individual patient basis.
3) the amount of fat that is obtained from perioral light perception is never going to be enough to do an adequate amount of upper eyelid fat grafting. To do upper eyelid fat grafting, particularly worth combined with nasolabial fold grafting requires a separate harvest site as at least 15 to 20 mL of fat need to be harvested.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had double jaw surgery on June 3 and am unhappy with the results. I feel like my maxilla was not moved forward nearly enough, and my bottom jaw keeps trying to move further forward but the maxilla is in the way. The surgeon brought the maxilla down when I think it should have been brought up and forward. I am interested in fixing the issue but really don’t want to do another full hospital stay- are you able to do an in-office le fort I with local anesthesia? I know this is possible in other countries. Otherwise, what options do you think I have? I am concerned with both function and aesthetics, and I feel that both are lacking.
A:I would never do or even attempt jaw osteotomies under local anesthesia. Now that the bone cuts have been made and plates applied you could do the procedure under general anesthesia as an overnite patient in a surgery center.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I came across your contact information online. After reading your reviews, I decided to reach out to you regarding the possible removal of an occipital fold procedure.
A:Thank you for sending all of your well illustrated pictures. As occipital scalp rolls go yours is a fairly minor one in terms of the magnitude of its size. It does not have an associated overhang which is what occurs in larger occipital scalp rolls.. This raises the question of whether the scar trade-off would be favorable, meaning is a fine line scar across the lower back of your head better than the appearance that the fold has now. Of this I am uncertain even though this is an individual patient judgment. But it is important to remember that once the scar is createdm there is no magical eraser to remove it later if one does not feel it was a worthy trade-off.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to know if the doctor preforms a surgery to fix a deformity of the ribcage like barrel shaped ribcage thanks I’m willing to go for a very aggressive risky approach as long as it provides a real change im tired of living with this deformity its impacting my quality of life in every single way my hurts from hunching it all the time trying to hide my protruding barrel chest it’s just unacceptable and very unappealing.
A:In the barrel chest deformity it would be necessary to do rib reduction osteotomies at multiple levels probably from rib # 5 down through #9. The question is not whether this can be done but how effective would be in doing so. To my knowledge no one has ever performed such a procedure before so knowing how effective it would be remains speculative. The unknown variable in removing lateral rib segment at this level of the rib cage is how much flexibility of the ribs exist, in other words can you close down the resected rib ends and put them back together and , if so, how large of a rib segment can be safely removed. I know from doing rib reduction osteotomies at rib #9 that at least one cm of rib bone can be removed and the two ends plated it back together. But does the same rib flexibility exist as you go higher up on the ribcage? For now we can only speculate that it does but until the surgery is attempted no one can answer that question with certainty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I am considering facial contouring procedures and wanted to ask specifically about reducing the width of my face. Would it be possible for you to let me know if decreasing my face width is feasible in my case, and if so, by approximately how many millimeters it can realistically be reduced? I am planning to do around 5mm on each side, and I would like both bitemporal and bizygomatic length be reduced. Also, I would like to ask if buccal fat removal, alarplasty, epicanthoplasty+lateral canthoplasty, and lip lift/philtrum reduction can be done altogether in one surgery
A: Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) in terms of bony facial width reduction, otherwise known as cheekbone reduction osteotomies, you certainly can get 5 mm per side of bizygomatic width reduction. When it comes to bitemporal width reduction that answer depends on whether you are referring to anterior or posterior temporal reductions. Most likely based on your desire for a facial with reduction you are referring to the anterior muscle compartment. Of that you cannot really reduce that area particularly above the zygomatic arch. There is no good method of anterior temporal muscle reduction particularly closer down to the level of the bony zygomatic arch we’re the greatest thickness of the muscle exists.
2) it is common for buccal lipectomies, nostril narrowing, lateral canthoplasties/epicanthoplasties and subnasal lip lifts to be performed in a single surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I want to reduce he “vertical height” of the anterior nasal spine, which is what I was asking if could be reduced/shaved from the bottom. This would help reduce the total nose height of the face.However, this might reduce the bone support for the Nasal Columella. To which I proposed if, a bone graft or cartilage could be used on the top of the anterior nasal spine, hence increasing its vertical length again but this time on the top. And then a rhinoplasty is performed. In this way, theoretically, the nasal height was changed but the bone support and the nose shape etc are still ideal. This surgery also in turn could help us in improving other craniofacial measurements like the length of midface (this theoretical reduction of nose height will increase philtrum height which we can again decrease with a lip lift thus reducing the midface length).
I just wanted you to ask you if this is possibly even THEORETICALLY, I’m aware that no surgeons have ever done it officially.
A:Thank you for your clarification on your surgical objectives. I don’t think the question is whether such an operation can be technically done as it is fairly straightforward as you have illustrated despite the fact that it probably has never been done in exactly the way you have described. My concern would not be whether it can technically be performed but whether in so doing the aesthetic outcome is exactly what you think it may be. The problem is you’re making a lot of assumptions about the aesthetic outcome based on drawing on a skeletal model. That is often a flawed concept as what happens at the bone level does not always translate to the outward aesthetic effect. One major consideration is that if the objective is to reduce mid facial length that is simply never going to happen no matter what you do at the bone level. Everyone fails to factor in to what happens to all the overlying soft tissue no matter what you do to the bone… It does not go away and thus external mid facial length is never really changed. The only effective mid facial length reducing procedures are sub nasal lip lift and reductive rhinoplasties that are associated with increased tip rotation. Nothing you can do at the bone level is ever going to decrease external midfacial length.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had a genioplasty last year and then a revision earlier this year. I developed a deep mentolabial surcus that I never had before in my life. I’m so unhappy with the look of this sulcus or crease and I think it looks so masculine. I just hate how my chin looks in general. I think my chin looks unrefined and like a block. I think I was expecting it to look like an implant with a more elegant curvature and definition. Is there anything that can be done about A) the sulcus. Would it be possible to soften it? I also have developed chin ptosis and it looks just awful when I smile or talk. How is that treated permanently? Can a lower facelift get rid of all of that sagginess? Is it possible to surgically remove the extra soft tissue that has formed. I really appreciate your advice
A:Based on your postoperative pictures, and I have no idea what you look like before the surgery, this looks like a perfectly normal postoperative result from a sliding genioplasty. I don’t find the labiomental sulcus to be particularly deep and I don’t see any way to take that sulcus and make it less deep. As a general rule and a sliding genioplasty the shape of the chin from the front view usually gets a little bit more narrow but not wider. I suspect what you do not like about this result is that you probably were seeking a more V-shaped chin which could only really have ever been achieved by a V shaped chin implant that does not have any wings. While I obviously have no knowledge about your preoperative discussion with your surgeon but based upon this outcome and your issues with it this was simply not the best chin procedure for you given what your chin shape goals were. A sliding genioplasty is usually not a good choice when one wants a very controlled shape to the chin.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
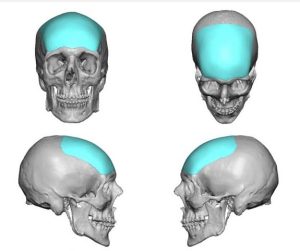
Q: Dr. Eppley, I wanted to inform myself about what you can do aesthetically to a skull. I am a 28-year-old man. I was born with a broad skull, or in medical terms, brachycephaly. My question is: what can I do about this later in life? I would like to have surgery. The reason is that this condition weighs heavily on my mental well-being. I don’t go out much anymore because I’m so insecure about it. I used to be able to partially hide this with long hair, but I started losing my hair a year ago, and it’s no longer hideble. My head is spread out to the sides and my head is flattened at the back Attached is a photo of what my skull looks like. I hope to hear from you. Thank you in advance!
A:Thank you for your inquiry and sending your pictures. You have a classic case of aesthetic brachycephaly with a flattened back of the head with a widened parietal – temporal sides of the head. The most practical procedures for improvement would be a custom scholar implant for the back of the head and reduction of the sides through a temporal reduction procedure. Ideally you would like to reduce the temporal– parietal bony eminences as well but I don’t think that aesthetically justifies a vertical incision over that area. The temporal reduction procedure is essentially scarless within an incision on the back of the ear in the crease.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, So my actual face is like the attached pictures.But I desire a look similar to this picture
My bite is perfect I just need the change for aesthetic purposes.. Do you think Bimax is the best solution or implants?
A:Based on your face now and your desired goals double tall surgery with absolutely not be the correct procedure. Your most major skeletal deficiency is in a very short chin with indistinct Jaw angles. That is best addressed by a sliding genioplasty combined with a wraparound custom jawline implant. Your chin deficiency is significant and is probably in the 12 to 14 mm range she’s beyond what an implant alone should do. The jawline behind it however can only be augmented with implants. Therefore you combine the two concepts into a sliding geniopolasty with the custom jawline implant that blends into it and creates a total overall jaw augmentation effect.
Your mid face only lacks some cheekbone prominence well the rest of it has adequate horizontal projection. Therefore this can only be addressed by an implant approach.
As you have already stated your bike is perfect and your concerns and not functional.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in getting implants for my very flat butt. I have attached pictures so you see what I mean?
A:Thank you for sending your pictures. You have a buttock shape that poses significant challenges for improvement. You have a very long buttocks with a low infragluteal crease but a flat shape. This cannot be treated by implants alone as implants only affect the top to middle portion of the buttocks and not the lower third. In the long buttocks patient with a very low infragluteal crease a lower buttock lift/tuck is initially needed to shorten it’s vertical length and provide a better demarcation between the buttocks in the posterior thighs. Buttock implants can then be done secondarily and will look better.. I have combined these two procedures in the past but inevitably it results in undesirable infragluteal scarring and I have learned that it is best to stage it in the vertically long and flat buttock patient.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I hope you’re doing well. A year later after the occipital skull reduction procedure I’ve finally shaved my head and I’m fully satisfied with the results – however, there is a persistent discolored red splotch of skin surrounding the left side of the incision scar – at first I thought I just irritated the skin shaving it, but it hasn’t gone away. Do you know what it could be and if so, is there anything I can do about it?

 A:Thank you for the long term follow-up which is now over one year from your occipital skull reduction. In looking at your picture the actual scar line is so minimal that it really cannot even be seen. There is, as you have pointed out, and overall reddish discoloration to some of the surrounding scalp skin. This is not really part of the scar per se but is some generalized scalp skin vascular dilatation. That is not a postoperative phenomenon that I have ever seen before or has been reported to me before from any type of scalp incision from skull reshaping surgery. Despite its rarity the treatment of it is not rare. Such vascular skin issues are typically treated with a tunable or pulse dye laser adjusted for the wavelength and color of the lesion to be treated. Such tunable wavelength lasers have been around for over 30 years and their initial introduction of use in the 1990s was for a more severe type of vascular anomaly, the port wine stain. Whether it be a port wine stain, telangiectasias for a generalized vascular rash this type of laser treatment can be very effective at reduction of the color.
A:Thank you for the long term follow-up which is now over one year from your occipital skull reduction. In looking at your picture the actual scar line is so minimal that it really cannot even be seen. There is, as you have pointed out, and overall reddish discoloration to some of the surrounding scalp skin. This is not really part of the scar per se but is some generalized scalp skin vascular dilatation. That is not a postoperative phenomenon that I have ever seen before or has been reported to me before from any type of scalp incision from skull reshaping surgery. Despite its rarity the treatment of it is not rare. Such vascular skin issues are typically treated with a tunable or pulse dye laser adjusted for the wavelength and color of the lesion to be treated. Such tunable wavelength lasers have been around for over 30 years and their initial introduction of use in the 1990s was for a more severe type of vascular anomaly, the port wine stain. Whether it be a port wine stain, telangiectasias for a generalized vascular rash this type of laser treatment can be very effective at reduction of the color.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have a question pertaining to facial implants and specifically medpor cheek implants, if someone were to have these types of cheek implants, can they then have fat grafting on top?
A: Yes, provided the injector knows they are there and doesn’t inject into them.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I am considering undergoing mouth widening surgery sometime within the next year, along with some other procedures. I would like to know how much scarring to expect and the probability that I will need scar revision surgery.
A:It is always wise in a procedure like mouth widening surgery to be aware of the scar and that potential need For scar revision surgery. I talk about it all the time because the corner of the mouth is a particularly challenging area for scars due the intersection of the upper and lower lips. This results in stretching of these lip corners that results from mouth opening particularly when that corner is expanded as in mouth widening surgery. It is also important to remember this is not just one surgery but there are two separate mouth corners which really makes it a bilateral or double procedure. This elevates any potential risk for adverse scarring x 2. Invariably when there is a scar issue it is almost always on just one side and the other side is acceptable.
 That being said having done many mouth widening surgeries the actual number of patients who request or go through scar revisions is relatively low. Butt low should never be misconstrued as never can happen as that is the risk of the surgery. Attached is a representative example of a mouth corner scar in which the patient had no concerns.
That being said having done many mouth widening surgeries the actual number of patients who request or go through scar revisions is relatively low. Butt low should never be misconstrued as never can happen as that is the risk of the surgery. Attached is a representative example of a mouth corner scar in which the patient had no concerns.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I came across your name while researching online. I am living with multiple familial lipomatosis. My lipomas started appearing about ten years ago, and their number and size have gradually increased over the years. The largest and most bothersome ones are located on my thighs.I am currently followed by my general practitioner, but according to him, there is nothing to be done as this condition is benign.
It is becoming increasingly difficult for me to live with this condition and carry out daily activities. I read that you offer solutions such as SmartLipo or other less invasive methods than conventional surgery to remove or reduce the size of lipomas. If you can help me with this condition, or refer me to a plastic surgeon in Canada who could perform the same type of procedure, I will pay for your services and advice.
Thank you, and have a great day.
A:Thank you for your inquiry and describing your lipoma condition. Having treated numerous familial lipomatosis patients it is a symptomatic approach rather than a cure. In most cases you try to do as many as you can, in which I have done up to 100 lipomas excisions in a single patient. While non-excisional methods may be used in the patient with discreet lipomas whose primary goal just to avoid scar this is not an approach that I will use in the familial lipomatosis patient. There are simply too many of them and such non excisional approaches leave behind some of the fatty tumor and most importantly, its vascular pedicle, which only means the risk of recurrence is high. Well I never like to place multiple small scars in a single area the familial lipomatosis patient is a lot more accepting of such scars given their condition.
This type of excisional surgery is tedious and I am not as enthusiastic about doing it as I have done in the past. But I need to take a look at the assignment to see how extensive it is. Since the most problematic ones are on your thighs please send me some pictures of your thighs at your convenience for my consideration.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My goal would be to fill in my undereye to a natural degree after getting cheek implants.? My eyes are very hollow so I happy with my cheeks that I have now have volume there. My surgeon said that the cheek went up to my under eyes and should fill it, which was the main reason I did it, but I’m still hollow. My surgeon said he could fill it in other ways at three months post op, but I tried filler years ago and it didn’t do much to fix the hollowness.
A: Thank you for sending your pictures. It is important to realize that with the use of standard cheek implants they are not going to provide any infraorbital or under eye augmentation. In the patient who has under eye hollowing who gets cheek implants it is going to magnify the existing under eye hollowing by virtue of augmentation around and below it leaving the under eye hollowing behind so to speak. Infraorbital augmentation can certainly be done with indwelling cheek implants in place. This requires a custom infraorbital implant design to both augment the infraorbital area as well as to blend over and merge with the existing cheek implants which will be seen in a 3-D CT scan which is necessary for the implant designs.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley,I came across your webpage on temporal width and zygoma reduction surgeries and had 4 questions about these procedures.
I am looking to reduce my bizygomatic width as well as the width of my face above the zygomatic arches, and saw that you previously wrote 7.5mm per side maximum can be reduced in the zygomatic arches so I was wondering what might affect this maximum between individual skulls, since I am concerned that in my case it may not be possible to achieve the reduction in width I want (roughly 7-8mm both sides) as well as if moving the arches inwards too much would cause issues with the temporalis or masseter muscles below.
I was also wondering with regard to the temporal width surgery, if you ever reduce the bone underneath, since my temporal fossa bulges more in comparison to the typical flat shape (I attached an image from my CT scan to demonstrate this), as well as if you are limited to reducing the posterior part of the temporalis.
A:In answer to your questions about facial with reduction:
1) I have yet to see any impingement on the temporal muscle from cheekbone reduction osteotomies no matter how much it is moved inward. I suspect this is due to the overlying fascia of the temporal muscle. The bone can be pushed inward as far as being up against the fascia but it can move no further. The temporal muscle lies inside the fascia, as a gliding muscle, is therefore not impinged. This is very different from zygomatic arch fractures in which the sharp end of the fractured bone penetrates the temporal fascia and induces muscle pain and the potential for mobility restrictions.
2) the facial/head width reduction surgery almost never is the temporal bone reduced. This is for one main reason and that is of access. Short of a bicoronal scalp incision there is no way to easily access the bone to do so. So even if one may benefit from temporal bone reduction the trade-off would be the fine line scalp scar from ear to ear across the top of the head. The scar issue aside coming from above would certainly maximize the movement of the zygomatic arch inward, perform some reduction of the thickness f the temporal muscle as well as reduce the thickness of the temporal bone.
In summary the scarless technique, coming externally with arch osteotomies and some muscle reduction, may achieve your desired results but let’s assume that while improved it cannot reach your ideal goal. Conversely the coronal scalp approach maximizes what is obtainable and would be much more likely to hit your ideal aesthetic target. In the end it comes down to how much effort are you willing to put in for what type of aesthetic outcome.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My nerve was damaged in my shoulder and killed my front deltoid muscles. I would like to get this to match my other shoulder.
A:Thank you for your inquiry and sending your picture. What you have is a classic example of deltoid muscle atrophy due to a motor nerve injury. It appears based on this one picture that only two of the heads of the deltoid muscle or involved (anterior and central) and that the posterior deltoid muscle head may have been spared. This is why you referred to it as the ‘front’ deltoid muscle.
That being said an implant would be the only way to restore as much as possible the volume from the lost muscle. Such implants can be designed several ways but the most common method, given your geographic separation, is by having you take measurements of its length and width from which I can make the computer design for the implant.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am scheduled to have clavicle lengthening surgery next month. I wanted to ask about the possibility of permanent loss of motion and function in my arms. An orthopedic surgeon friend recently warned us against this surgery, stating “this does not ‘simply make your shoulders wider’–it permanently rotates your shoulders into an abnormal position and you will loose motion and function.
A:Thank you for your question. In my experience that statement by the orthopedic surgeon is unfounded. That might be true if the clavicles were significantly lengthened by many inches per side, which I doubt that would happen even then, but that is not the amount of lengthening which can be done. I don’t know the basis of the orthopedic surgeon’s statement but unless he has done the actual surgery and seen that happen that is a conjecture and not a documented outcome.
Rather than that expressed concern the real potential complications of the surgery are nonunion of the lengthened bone, hardware loosening, and secondary surgery for these potential problems. Clavicle lengthening is very different from clavicle reduction due to the limitations the soft tissues of the shoulder. Thus the gains to be had, with a low risk of potential complications, is not to try to do too much lengthening. This means keeping the lengthening per side 2 cm or less based on how much the soft tissues of the shoulder will allow the bone to be lengthened. I suspect the basis of the orthopedic surgeon’s comments come from the belief that much more clavicle lengthening can be accomplished then what can actually be done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley ,Hello! I have tear trough implants that are not the same size. I was wondering if there was a way to have these implants removed and replaced with cheek implants.
A:The tear trough implants that you have are undoubtably made of silicon which makes their removal fairly straightforward. They can be removed by the same pathway in which they were placed. It is possible if they were sutured into place and not screwed into place that they can be removed intraorally. This would be compatible with your stated desire of cheek implants replacements in which most standard cheek implants are done intraorally. However if it is a custom infraorbital-malar implant, which is a typical midface augmentation area for men, it would need to be done through the lower eyelid which is probably how was your original teardrop implants replaced.
These are some general comments in regards to your questions but more specifics as they apply to your exact aesthetic midface needs requires a picture of analysis and further discussion.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I have a jaw contouring/ jaw reshaping concern. My right side lower jaw is bigger and draws the right side of my face downward. This is clear when seeing my lips, as the right side of the lips are pulled in a downward angle. It’s fairly clear to me that the right-side lower-jaw is overly large and extends excessively downward. Please let me know your thoughts!
A:As you have correctly surmised your jaw asymmetry is due to the right side being lower. This is a very typical form of Joel asymmetry and, for whatever reason it is usually the right side which is lower. The only effective treatment is an inferior border shave on the right side. This requires some x-rays for proper planning. At the least a Panorex X-ray will clearly show how much lower the right side is from the left as well as the location of the nerve as it runs through the lower jaw. This is known as the inferior alveolar nerve which supplies the feeling to the lower lip and teeth. This runs directly through the bone in the middle of the lower jaw and exits anteriorly through the mental foramen. Usually when the Joel is lower so is the nerve in the bone and we have to know exactly where that is to avoid injuring it in any type of bone removal. Most likely given where your jaw overgrowth is the nerve is probably got a safe distance away. But it is obviously important to know rather than to guess.
That issue aside the more relevant issue is the approach needed to remove the jawbone. The Jolla angle poses considerable technical challenges for proper access. Since what is needed is a specific linear cut of bone from the back of the jawline forward to the point where it matches better to the opposite side the only way to do that is an external approach. This requires an incision at the back end of the jaw angle. The alternative is an intraoral approach but this places the bone cut at an odd angle, a nonlinear cut, and it is very hard to be exactly specific as to the resultant bone shape that is created. It creates a curved shape unless the bone cut is placed very high which would then make your right side higher than the left and just cause the reverse problem.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in paranasal implants. My goal is to normalize the central part of my face having an aesthetic outcome.
A:Thank you for sending your pictures. I would need to know exactly what you are hoping that paranasal implants can improve or resolve. When one says normalize the central part of my face that suggests to me to provide some additional projection around the lower central mid face which paranasal implants can certainly do. If the goal is to sit softener significantly reduce the presence of the nasolabial folds in that regard I would not be as optimistic in terms of the effects.
That being said, provided the primary goal is increased projection for undergoing the procedure, is whether one should use standard or custom implants. That decision requires a more in-depth conversation.
Dr. Barry Eppley
World-Renowned Plastic Surgeon