Your Questions
Your Questions
Q: Dr. Eppley, What materials available for implants? I see he uses a lot of silicone and was wondering why that is. I prefer different material would that be okay?
A: There are a variety of materials for custom facial implants including solid silicone, Omnipore/Medpor, PEEK, PEKK and titanium…each with their own advantages and disadvantages There is no perfect faciak implant material.
While patients and even most surgeons get caught up in the implant material properties on a handling basis, often with very erroneous perceptions in vivo, to the body an implant is an implant is an implant. It is still a foreign material and no material offers any different or superior biologic benefit.
What separates these facial implant materials is not their biologic responsesbut other features such as cost, design limitations, and ease of placement and revision/removal .
Given that the revision rate of any custom facial implant is in the 40% range (shocking to patients but true), the concept of ‘easy in, easy out and easy back in’ has great clinical merit. This is where solid silicone has a significant material benefit and explains its broader clinical use than the other materials.
That being said it does not matter to me what material a patient wants to use as I have placed and removed every implant material that is available. What I care about is that the patient understands the advantages and disadvantages of their material choice.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in feminization surgeries. I currently present male, and would like to do surgeries before moving on. Ultimately I would like to have a number of procedures, but have no idea about cost or insurance. I had gastric sleeve performed 18 months ago and have lost 100 lbs. 5′ 9″ currently 180 up from a low of 170lbs. 48 years old next month. Procedures i am interested in: Butt and hip augmentation. (Currently thinking solid implants are preferable to fat grafting) Floating rib removal and/or repositioning Mid rib(lower attached ribs) repositioning Clavicle reduction Liposuction. (Belly, upper/lower back, thigh..etc) Overall skin removal and tightening (belly, butt, thighs, lower, mid and upper back) I am willing and able to travel for procedures and recovery. I would really like to get info on which procedures can be done simultaneously and approximate cost. Would like complete as much at one time as possible. Would also be interested in FFS at a future time. Thank you
A: When it comes to body feminizing surgery you have one unique anatomic feature that separates you from most other patients…..the large amount of weight loss. (massive weight loss or MWL) This creates the need for numerous body contouring procedures (skin removal and tightening) that do not necessarily have feminizing effects but are more of a ‘reconstructive’ nature. As a result considerable thought must begin to both MWL and body feminizing procedures to create a staged surgical plan for maximum efficiency and effectiveness.
That process begins by looking at your body pictures from numerous angles (front, back and sides) for an initial assessment.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in replacing my PEEK infraorbital-malar implants as they don’t saddle the rim and as a result they stick put unnaturally. These implants were placed intraorally at the time of double jaw surgery.
A: Be aware of two very relevant aesthetic issues. 1) when have to saddle the infraorbital rim you have to use a lower eyelid incision to do the dissection needed as well as to ensure proper placement and 2) PEEK is not a good implant material for thin tissues like the lower eyelid and orbital rims as it can not be made withj feather edging as it is machined in its fabrication. You will likely end up with visible edging even if it saddles the rim. …less than what you have now just at a different level and degree
There is a reason your current PEEK implants don’t haver a feathered edge design and look bulky…which is very obvious in bot the design and after actual placement. This is a design limitation of all very rigid materials that have to be machined in manufacturing. There is always going to be at least a 1mm edge. This is not an aesthetic issue in thicker tissues like the jawline and lower cheeks. But it will be one around the orbital rim which is an unforgiving implant placement site.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a separate medical enquiry, regarding bone burring to correct the prominence of my forehead. Can this be done please. Not sure if I’m imagining things but my right side seems to appear a bit smoother than the left, so it’s this left side I would’ve wanted addressing.
A:Are you referring to the prominence of your forehead or that of the brow bones. I ask because I don’t see any true forehead prominence. The other issue is for any forehead work where is the scalp incision going to be placed to do it. In the male with short hair here is no aesthetically hidden place to put it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley I hope this email finds you well. I’m reaching out to ask about surgery for the two horns on my forehead that stick out noticeably. I’ve attached a recent photo to show how they usually look.
I have a few questions:
1. How is the procedure done?
2. How much does it typically cost?
3. Will I be able to safely play soccer afterward, especially since I frequently head the ball?
I’d appreciate any details you can provide and look forward to your guidance.
Thank you for your time and expertise.
A:Forehead Horn reduction is typically done by bone shaving through a small scalp incision. In very large forehead horns like yours the key question is whether the bone is thick enough in the horn area to permit an adequate reduction. This requires a CT scan to make that assessment. Provided reduction can be safely done there would be no postoperative limitations in terms of playing soccer or any other activity where trauma to the head can occur.
The CT scan can be done in our local area and we provide the order form at a local imaging facility to have it done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m planning to have a genioplasty with you this spring and had a few questions about the healing process.How long does it usually take for the chin bone to heal enough to avoid bending in case of trauma.Would it be around 2, 4, or 6 weeks post op?
A:The chin bone is generally healed enough after 6 weeks that trauma to it would not change the bone position.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have very thin lower forearms from the wrist back. I know it is possible to have implants to the upper forearms but would the dr be able to use implants to thicken the lower forearms?
 A:Your pictures show a lower forearm deficiency which is most apparent in the dorsal position. (as you have shown all pictures from that perspective) Between largely being a dorsal deficiency and not having to cross the wrist this is a favorable area for implant augmentation. These would be suprafascial implants that wrap onto the volar part of the forearm which are ultrasoft with very feathered edges. (see attached picture) These would be made by taking measurements of the lower forearm area that needs the augmentation. (you can take the length vs width measurements) This procedure would be performed under local anesthesia.
A:Your pictures show a lower forearm deficiency which is most apparent in the dorsal position. (as you have shown all pictures from that perspective) Between largely being a dorsal deficiency and not having to cross the wrist this is a favorable area for implant augmentation. These would be suprafascial implants that wrap onto the volar part of the forearm which are ultrasoft with very feathered edges. (see attached picture) These would be made by taking measurements of the lower forearm area that needs the augmentation. (you can take the length vs width measurements) This procedure would be performed under local anesthesia.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Can Botox effectively reduce the size of the temporal muscle long term?
A: No, its limited effects are temporary.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q:Dr. Eppley, I am scheduled to have braces on the 30th can or will that interfere with cheek implant surgery?
A: No it will not. Braces in the teeth do not get in the way of intraoral access for the placement of cheek implants.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a previous patient of Dr. Eppley (Sept 15, 2022 surgery date). That procedure involved a surgically implanted plate and screws.I have an upcoming MRI and I need to confirm what implant material Dr. Eppley used, to be sure that it is completely MRI-safe and not at all magnetic. Can you check with Dr. Eppley and your documentation to find out?
Thanks for your consideration,
A: All metal implants used in the face since the early 1990s is made of titanium, a non-ferromagnetic metal.Thus any metal hardware implanted in your face would be MRI compatible.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, im interested in custom implants to make my masseter muscle bigger. I already have a jaw implant inserted because my jaw was shaved a decade ago and it ended up being a bad choice. Along with the jaw shaving they ended up shaving a good amount of my masseter which I desperately want the appearance of back. My face was much wider and now it is narrow. I have had fat taken out of my face, so im not talking about that, but the overall shape of the face. I last picture is the look i’m going for.
A: The challenge that you now have is that adding implants to the implant you have in place would be very difficult from an intraoral perspective. That is clearly a titanium or PEEK implant material in which fixing an implant onto it would be difficult. This is best done from an external approach where implant placement and fixation would be more assured.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Im wondering if I can get Kybella after a custom wraparound jaw implant?
A: Yes you can. Since Kybella is usually injected into soft tissues to reduce fat under which implants do not lie they would be perfectly safe to use.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I’m interested in 5mm mouth width expansion per side, I was wondering how long it would take for “normal” scarring that usually happens as a trade-off to look acceptable enough to not have it be easily noticeable by other people or distract from the result.
A: Corner of mouth scars generally take 3 to 4 months to mature particularly in intermediate skin pigments.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in revision options for my custom jawline implant. During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision. One option involved adding additional components to the existing implant to enhance projection and angles. He also suggested a soft tissue graft to address and cover the bulging near the masseter muscles.
Could you please provide more details about this approach? Specifically:
• Would the current implant need to be removed to incorporate the new components, or can they be added without removal?
• How are the additional parts secured—are surgical screws or adhesive methods used?
A:‘During my last discussion with Dr. Eppley, he mentioned several options beyond a full revision’
FYI it would be a full implant replacement….not a revision. A revision is when you are taking what you have and try to modify it. Plus a revision relates to the primary surgeon wo did the original work. When a new surgeon assumes that initial work it is a secondary procedure not a revision. While a bit semantical there are very different implication between the two.
‘One option involved adding additional components to the existing implant to enhance projection and angles’
 You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
You are referring to Transcutaneous Soft Tissue Jaw Angle Implants. A common technique that I employ to treat masseteric muscle dehiscence with implant reveal. It is the only technique that works if one desires to keep their current jaw angle implant shape. The alternative is to change the implant with a new design that doesn’t have such a square jaw angle shape…which is what caused the problem in the first place.
Soft tissue jaw angle implants are placed in the soft tissues overlying the current implants, they are not bone implants. (see attached picture)
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in Lefort 1 osteotomy surgery. The reason I want to have this surgery is that the maxilla, the middle part of my face, is long and I want to make it look shorter. My face, which is between the eyes and the lips. how much of a change there could be?
A: You are under a common misconception that if you shorten the maxillary bone (LeFort I impaction) your external midface appearance will get shorter…which it will not. The LeFort I impaction is for the treatment of the excessive gummy smile patient to achieve less tooth and gum show. It can not shorten the appearance of the midface as where does all the soft tissue go if the bone is shortened? It doesn’t go anywhere…it will remain the same.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What is the recovery time for temporal muscle reduction? I suffer from migraines a lot, would Botox injections help shrink the temporal muscle?
A: It takes a good 2 to 3 weeks for the swelling to resolve. But there are no physical restrictions during the recovery.
My assumption in your questions is that you may be seeking temporal reductions for migraines?? If that is the case the important question is where is the location of the migraine pain in the temporal area? Knowing that information will determine whether surgical reduction or Botox is the appropriate treatment.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
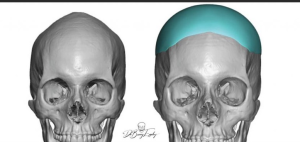
Q: Dr. Eppley, I’m interested in aesthetic skull reshaping surgery & the costs involved. I’ve attached a few photos to see of the desired “after” results are possible and what costs would be involved.
A: Based on your own imaging it appears that you have done a modest left forehead-parasagittal augmentation. This would be very achievable as with a 3D Ct scan one could see the difference between the two sides and from that difference a small custom skull implant can be designed/made to provide a symmetry-achieving effect.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi Im very interested in ZSO on my right cheekbone to expand and match my left.
A: The main concept to grasp is that when one side of the cheek is asymmetric (smaller ot bigger) it is a three-dimensional problem not a two dimensional one. The cheek is a solitary projection from the side of the midface so there is more than just a width deficiency when it appears amaller. The zygomatic sandwich osteotomy (ZSO) creates a two dimensional effect not a 3D one. This will likely become glaringly apparent when the ZSO operation is performed. This is why a 3D cuystoim cheek implant produces a better aesthetic result from all facial angles.
But even if a ZSO is to be performed the critical question is how much expansion is needed to optimie cheek symmetry. This is where a 3D CT scan of the face is needed to determine not only how much width addition is needed but how significant the 3D bone differences are
Dr. Barry Eppley
World Renowned Plastic Surgeon
\
Q: Dr. Eppley, I am interested in changing the shape of my head. Attached below are two pictures of me and 3 picture that I can find to best describe what I want. Hope this helps.
 A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
A: Based on the pictures you have sent you appear to have an inverted V shaped top of the head with narrow sides. (parasagittal and temporal deficiencies) The two skull implant shapes you have shown are designed to address those goals and can be placed during a single surgery.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi!! I just heard that dr barry eppley had done inferior orbital box osteotomy, which is less riskier than 360 degree OBO. Actually i just wanna reduce my IPD as a woman. Can this technique reduce my IPD by upto 5 mm. Also can Dr. Eppley perform it?
A:Inferior box osteotomies can be effective for modest IPD increases but not for IPD decreases.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I was looking at some videos on youtube of Dr. Eppley performing this procedure and I was wondering if the implant that is slid under the skin on the scalp could cause some kind of damage to hair follicles?
Also once the surgery is performed could the implant move? If the back of the head was to be hit or hit some sort of surface could the implant be displaced under the skin?
Would wearing a motorcylce helmet also potentially cause this? Or other complications?
A: 1) The implant is placed on the bone under all five layers of the scalp way under the location ofmthe hair follicles. As long as the patient doesn’t insist on having an implant that is too bog there is no excessive stress on the hair follicles. (shock loss)
2) Because of their large surface area coverage and the tightness of the overlying scalp skull implants can never move or change position.
3) Skull implants are impossible to fracture or be damaged. As a result ther are very much like putting a bumper on the skull….providing inadvertent protection to the skull from any future trauma.
Dr. Barry Eppley
World Renowned Plastic Surgeon
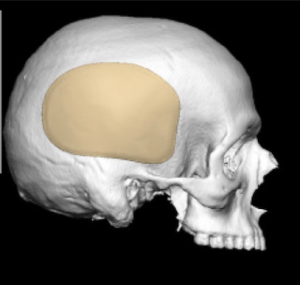
Q: Dr. Eppley, I wanted to do plastic surgery on my forehead.
A: I believe you are referring to the bony prominences of upper forehead known as large forehead horns which is a form of frontal bossing. How successfully they can be reduced depends on the thickness of the upper forehead bone which requires a CT scan to determine. (how much the bone can be safely reduced)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in Skull Reshaping. Although I am a petite person, I feel that my head is too small head and would like to add some height and volume to the crown of my head. What is involved in this surgery and how safe is it?
A: You are referring to classic female crown of the head augmentation nusing custiom skull implants which I do regularly. There is no question about safety of the surgery. The more pertinent question is whether your desired result requires a one or two stage skull augmentation approach. (the latter is what most females need to achieve their desired result)
I would need to see some head pictures for an assessment and imaging to help make that determination.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, isis any type of procedure that can shorten the midface area? I am assuming no because I already had double jaw surgery 8 years ago and cannot have any further orbital surgeries due to my surgical history.
Is a custom supraorbital/infraorbital implant something that may improve the eye area appearance compared to my current fillers and implant
The main thing I am unhappy with is how my eyes look when looking downward – the hollowness and sunken space above my eyes – maybe a better supraorbital implant would help
In regards to the rest of the face – shortening my midface and maybe a slightly wider and longer jaw
If the midface cannot be shortened I am assuming that lengthening the jaw a little bit will make it look more proportional.
A:You have correctly surmised that you can’t vertically shorten the midface. What can her done is to vertically lengthen the lower third and mildly augment horizontally the middle third as in the attached imaging.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I contacted a couple of months ago about clavicle reduction surgery as a trans woman 28 with large shoulders at the beginning of transitioning. I was hoping to get a consultation to discuss this further and if you have done any manipulation or reduction of the scapula as my shoulders are so broad and it’s one of the biggest parts of distress to me and really really need help with this. I’m not fully committed yet, but I still would like to pay for a virtual consultation as I really would like to discuss my concerns.
A:While scapular spine reduction can be concurrently done in shoulder reduction surgery for its prominence you are probably referring to the width of the scapula for which there is no satisfactory reduction technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Would temporal artery ligations be covered by insurance?
A:That is a question to which the answer I would not know. But I would highly suspect unless their were medical symptoms associated with it (e.g., autoimmune, visual impairment) that it would be viewed as a cosmetic issue.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I have attached pictures of my penius both erect and flaccid. I suppose this sort of surgery is always for aesthetic reasons, but I feel the need to justify anyway. :-)In the flaccid picture I just feel that the scrotum is smaller than it “should” be proportionally. I realize this is because I have an above average flaccid length that varies but with the suprapubic area retracted (as I am hoping it will be post lipectomy) the flaccid length is in the neighborhood of 6 or 7 inches. The skin tightening will draw the scrotum up more and I would prefer the scrotum to hang down at or even past the length of it flaccid. That just seems like the traditional shape in my head.
The “problem” is exacerbated when I become erect as I believe they become very much dwarfed by the rest of my shaft both in girth and length. If I am not explaining myself well, please feel free to ask questions if it will get more useful information.
The last picture is sort of a goal picture. It is of me a day or some after having infused about 750ml of 0.9% Sterile Saline IV Fluid. (I take every precaution imaginable.)
A:This is classic aesthetic penile-scrotal disproportion. When it comes to testicle implant size selection using a side by side or displacement technique here are the concepts to know:
1) It is not an exact science. Until one is in surgery there is no way to know what will ‘fit’ or what the maximum implant size the scrotum can handle. There are no preoperative measurements/tests that will answer that question.
2) But since every testicle implant over 5cms in size must be made custom we do have to pock a size since it is one custom design per patiebnt.
3) A good rule to follow is that for adequate displacement of your natural testicles the implant should be at least 70% that of your natural testicle size. (100% is even better)
4) If any custom testicle size that is chosen does not fit in surgery I can manually reduce them so that they will. (would like to obviously avoid)
5) ) Many custom testicle implant size selections are a battle between myself (who is worried about having them fit and the creation of potential problems ) and the patient who wants the maximum size possible. (who is understandably only focused on the their benefits)
6) Your goal picture sh0w very low hanging testicle, which may or may not occur from large testicle implants, but most certainly will not in the early after surgery phase. That requires time and scrotal skin relaxation….and may well require ‘ball stretching’ postop as well.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I wanted to inquire about what I could realistically achieve when I commit to a full jawline implant and 2 cheek implants. I would like to restore what I had but wanted to see if it was possible without adding much vertical length. I feel that on the side that I liked the most they mostly took the jaw angle and the thickness of the bone. I wanted to attach pictures to have you run by Dr. Eppley to see if this is achievable. Additionally would it be better to have my zygoma knocked back to the original position and have standard cheek implants put in or will custom be better for adding width and projection back to my cheekbones instead of just forward projection. I am attaching the photos below. These are all before my jaw surgery in Korea. The first is what I had before and the second is the width from the side I liked.
Thanks for all your help!
A:In looking at your panorex xrays before and afters, which provide the best information we have as to what was actually removed in your V line surgery (3D CT scans are best), it can be seen that it was really in the jaw angle area where most of the bones was removed vertically. (the chin was spared) When reducing jaw angle length that also reduces jaw angle width. I see no bony reductive changes anterior to the jaw angles. Thus if the goal is jaw restoration, but without adding any vertical length, then it would be just adding back some width only to the jaw angles. Whether that amount of width reduction is worth a custom implant approach can certainly be debated.
For the cheeks you can’t just cut the bone and push it back out. Such cheekbone reduction osteotomies are a one way street so to speak. Cheek restoration requires an implant overlay. The debate there is whether standard or custom implants can do so better or more effectively.
While it is always hard to argue that custom implants are always better for any form of facial bone restoration that always depends on how much bone augmentation is needed, whether any significant asymmetry exists and what the patient prefers.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had double-jaw surgery some time ago to correct my short face syndrome. The swelling is almost all gone. While there has definitely been some improvement in the length of my face, I still feel that my chin is too short and I think I could benefit from another 4-6 mm of vertical height. But if you refer to the picture I shared, I think the way the surgeon has done the genio cut makes it difficult to get another vertical genioplasty. Am I correct?
A:You are correct in that with that genioplasty design it would be very precarious to try and do a secondary vertical lengthening genioplasty…not to mention the bony stepoffs would become much greater and noticeable with that osteotomy design. To achieve another 5mms of vertical chin lengthening you would be better served inferior implant augmentation, particularly a custom implant desitn to add length, smooth over the bony stepoffs and blend into the jawline behind the chin with smooth inferior border contour.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi there, I contacted a couple of months ago about clavicle reduction surgery as a trans woman 28 with large shoulders at the beginning of transitioning. I was hoping to get a consultation to discuss this further and if you have done any manipulation or reduction of the scapula as my shoulders are so broad and it’s one of the biggest parts of distress to me and really really need help with this.
A:While scapular spine reduction can be concurrently done in shoulder reduction surgery for its prominence you are probably referring to the width of the scapula for which there is no satisfactory reduction technique.
Dr. Barry Eppley
World-Renowned Plastic Surgeon