Your Questions
Your Questions
Q: Dr. Eppley, How long do skull implants last and are there any long-term side effects? And how much big cut is needed for a complete head augmentation?
A:Skull implants last a lifetime and never need to be replaced due to device failure as they are solid and do not degrade over time. Their effects are aesthetic in nature and they are not associated with any other side effects other than those that are associated implants placed anywhere in the body. The concept of ‘complete head augmentation’ can have different meanings but I will assume it is an implant that covers the majority of the skull in which case a near complete coronal scalp incision would be needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hope you are doing well! I was just curious, when you perform Adam’s apple augmentation, does the grafted cartilage heal and become one with the preexisting Adam’s apple? And just in case you’re able to answer this as well, is the cartilage is only grafted from the rib area? Thank you so much for all you do!
 A:When performing Adam’s apple augmentation there are two techniques to do so….rib cartilage (which is the only donor source that provides enough harvest material) and an implant material. (Medpor sheet) Since you asked about rib cartilage it is important to understand how rib cartilage (as well as all cartilage grafts) heal as it is very different than bone grafting from a biologic standpoint. Cartilage is an acellullar and inert tissue. Thus when it is grafted it is largely non-dynamic…meaning it just sits there. It becomes encased in scar but does not really blend in and become part of the natural cartilage bed on which it lies. Unlike bone it does not got through a process of breakdown and incorporation. Its remains fixed onto the site in which it is implanted but never becomes truly integrated into the recipient site tissues.
A:When performing Adam’s apple augmentation there are two techniques to do so….rib cartilage (which is the only donor source that provides enough harvest material) and an implant material. (Medpor sheet) Since you asked about rib cartilage it is important to understand how rib cartilage (as well as all cartilage grafts) heal as it is very different than bone grafting from a biologic standpoint. Cartilage is an acellullar and inert tissue. Thus when it is grafted it is largely non-dynamic…meaning it just sits there. It becomes encased in scar but does not really blend in and become part of the natural cartilage bed on which it lies. Unlike bone it does not got through a process of breakdown and incorporation. Its remains fixed onto the site in which it is implanted but never becomes truly integrated into the recipient site tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am experiencing some jowling in my lower face and my cheeks are slightly sunken. I still look okay, but tired some days. My face can seem drawn down with the mild aging. I am 51 and am trying to figure out the best solution. I am trying to decide among the following: Sculptra for my cheeks, Fat transfer to face (mainly cheeks), or a mini face lift just for the jowls. Cost is a factor, but I will consider financing. Attached is a fairly recent picture. Would you please help me with this decision. Anything you can provide information/estimate of costs would be appreciated. Thank you.
A:Thank you for your inquiry and sending your picture. You have mentioned two main areas, cheeks and jowls/jawline. In looking at the best ROE (return on effort) there is no question that the jowl tuckup procedure (aka mini facelift) would provide the greatest aesthetic benefit. This is what is creating the heaviness and drawn down appearance. You only consider Sculpra for the cheeks if surgery is not going to be an option. Fat injections is still a surgical procedure and would be done during a minim facelift so fat injections done alone seems the least likely of the options you have mentioned.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As a male I would like to increase the length of the skin of my upper lip as I find it too short. How could this be done?
A:You can not increase the actual external skin length of the philtrum. What you can do is roll out the internal mucosa of the upper lip (V-Y mucosal advancement) which can effectively bring down the central part of the upper lip smile line. This could also be combined with a lowering vestibuloplasty, all of which is designed to bring down the inner portion of the upper lip to cover tooth show at rest.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Hello, I got a buccal fat removal and I am not happy with the results my cheeks look hollow and I would like to see if there’s something I can do about it?
A: Since fat removal is the source of your now hollow cheeks, fat replacement would be the logical treatment choice. The debate for this type of far grafting is whether it should be done by injection vs an intraoral enbloc solid fat graft placement. There are advantages and disadvantages with either approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a couple questions regarding style 2 custom cheek implants. I am scheduled to have a rhinoplasty in November 2021 and hope to perhaps pursue cheek implants in 2022.
1. How long post-rhinoplasty do you recommend patients wait before getting custom cheek implant surgery?
2. In addition, can you provide an approximate estimate for the cost of style 2 custom cheek implants? Does cost vary depending on the size of the custom implants?
3. Can style 2 custom cheek implants also augment the cheeks, or are they limited to the infraorbital rim and zygomatic arch?
Thank you!
A:In answer to your custom cheek implant questions:
1) I would allow three months after a rhinoplasty to get any form of facial augmentation surgery.
2) The cost of style 2 custom cheek implants is the same regardless of their size or surface area coverage.
3) By definition a style 2 custom cheek implant is an infraorbital-malar implant style that augments the cheeks.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, how much shoulder width reduction s possible to reduce on a man? Just 1 inch or is it more? I work as a Speleologist/Spelunker and I would like my shoulders narrower for obvious reasons.
A: Shoulder reduction surgery reduces each side by 1.0 to 1.2 inches based on the patient’s height. This is the same for men and women.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to ask you just a very quick question about brow bone reduction surgery. I have seen all articles on your website related to this – brow reduction, contouring, augmentation etc. In my case it has to be definitely just brow bone reduction (like on the first picture you send me) But would you take a look at my picture again and tell me which method could work best for me. If it´s with a complete bone flap or without complete bone flap replacement, or even if in my case 2 mm endoscoping shaving can´t be enough. I don´t know, tell me which method you think could be best for me,,, and then we can set the conversation and plan the surgery, because I´m from Europe so it´s little complicated these times.
A: The brow bones are caused by an over expansion/aeration of the underlying frontal sinus cavity…thus much of the central brow bone is ‘air’ and only a thin covering of bone exists over it. Thus only 1 to 2mms of bone can be removed by shaving since one will thereafter create a large bone defect. Shaving would only be effective in your case if you were willing to accept half or less of the current imaged result. This is why the bone flap technique is almost always the best for men.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I have done extensive research and have discovered the genius Dr Eppley! I am very impressed with his work and also the army of positive reviews online about him.
Upon research, I also discovered he is an expert in custom jaw/chin + forehead implants- both which I am very interested in. Would it be possible for Dr Eppley to find a way to enlarge and round my forehead with a custom implant?
I have been getting filler in my chin and jaw for the last few years and have LOVED IT. Now I am looking for a more permanent solution with a possible custom jaw wrap if appropriate.
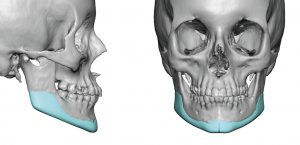 A: Thank you for your inquiry, sending your pictures and detailing your surgical history and goals. From a jaw augmentation standpoint you are correct in that a custom wrap around implant would be the ideal way to go. For females these are often more ‘petite’ type designs as one would imagine. The use of 4ccs of soft tissue filler is a good guide which translates to about 50% more volume when it is added down at the bone level and not into the soft tissue.
A: Thank you for your inquiry, sending your pictures and detailing your surgical history and goals. From a jaw augmentation standpoint you are correct in that a custom wrap around implant would be the ideal way to go. For females these are often more ‘petite’ type designs as one would imagine. The use of 4ccs of soft tissue filler is a good guide which translates to about 50% more volume when it is added down at the bone level and not into the soft tissue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in the total head widening procedure that you perform as I have a very rounded narrow forehead and browmridge and would like for them to be widened and advanced using implants.
More specifically, I was interested in this specific model shown on the website. What would the pricing of this type of implant be? Also, is there a threshold for the amount of implant that can be squeezed in? I would require a fair bit of advancement so I’d like to know what the limits of such an implant are.
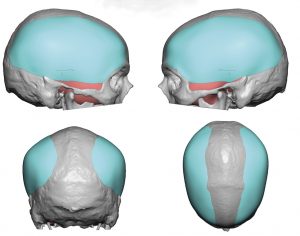 A: The limits of any skull implant is based on its volumetric expansion. As a general rule scalp stretch can accommodate up to 125 to 150ccs in most people. The specific forehead implant to which you refer is 104cccc with a maximum thickness of 6mms.
A: The limits of any skull implant is based on its volumetric expansion. As a general rule scalp stretch can accommodate up to 125 to 150ccs in most people. The specific forehead implant to which you refer is 104cccc with a maximum thickness of 6mms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m so impressed of your work to enlarge mouth, and I really want to do it for my mouth to make it wider (maybe 1″ would be the best).
As you can see in the picture, I have a ratio between nose and mouth around 1:1, which is not good and I can’t have a good looking smile.
A: There are two factors you need to consider in mouth widening surgery:
1) The maximum amount per side done is 7mms.
2) Scars at the mouth corners are unpredictable and there is a relatively high rate of revision of them.
Dr. Barry Eppley
Indianapolis, Indiana
Q:Dr. Eppley, For context, I am a healthy man in his early 30‘s who wants mild-to-moderate enhancement of the chin as well as the jaw angles in the lateral dimension. I am going for a strong but natural jaw appearance.
Regarding sliding genioplasty, what is the rate at which additional surgery is required, either due to functional problems (e.g. issues with talking or chewing, etc.) or inadequate cosmetic goal? Also, is it true that sliding genioplasty will yield a more natural look than a chin implant?
Regarding custom jaw angle implants, I am again curious about the success rate for the procedure. What is the rate at which they require additional surgery for any reason (e.g. needing to be taken out perhaps due to infection, revision surgery due to inadequate cosmetic goal, etc.)?
Thanks for the time you spend answering these questions. I am planning to make use of your services in the future.
A: Thank you for your inquiry and sending your pictures to which I can say the following:
1) Your chin augmentation would be best served by a sliding genioplasty because you need a combination of both horizontal and verticial dimensional increases…not because it looks more natural than a chin implant but because that is the safest method to do so with a small and tight overlying soft tissue chin pad.
2) The sliding genioplasty has a very low complication/revision rate in my experience. I have never functional issues like talking or chewing concerns as you have mentioned.
3) As for jaw angle implants the key question is whether standard or custom implants are needed and that would depend on one’s aesthetic goals which are yet to be determined. Unlike the autologous slidiing genioplasty operation jaw angle implants have a much rate of infections/asymmetries which is in the 10% range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I am very interested in your iliac crest reduction procedure, and was simply wondering: when you shave down the hip bone what happens to the muscle attachments that connect to it? Hope this isn’t an impossible question! Thank you so much.
A:What is released when you do iliac crest reduction, which is done only in the central wing of the bone, is some the TFL fascial attachments laterally and some fibers of the external abdominal oblique muscle medially. Once the bone is reduced, these two attachments are put back together to provide some additional soft tissue coverage over the reduced bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have scheduled an appointment for rhinoplasty with you in the fall. Not sure if this is a question I should send to you but you told me to reach out with any questions.
I just want to ask if this procedure would not only improve the tip appearance but the overall nose (nostrils etc.) my primary concern is the drooping and bulbous tip but I just want to make sure I understand.
A: Most nose tip reshaping changes do affect the nostril shape, usually favorably, particularly when a droopy and bulbous tip is reshaped.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My lower lip is slightly behind my upper lip maybe 2mm, I’ve had double jaw surgery in the past and it’s definitely better than it was, but it still bugs me and I find myself biting my lips a lot because of it. I know the only way too truly fix that is with a BSSO which I will get again in the future to fully correct it. In the meantime though I’m curious would filler be able too push it out a bit too meet the upper lip?
A: I would think it would as that is how injectable filler works…volumetric expansion of the injected tissues.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, We had a consultation a few months ago and I got X rays done locally (not the cone bean scan you requested but similar). I was curious if you see an issue with my airway, in that its very narrow? I was told this could lead to sleep apnea/other breathing problems and a jaw surgery could help remedy this.
A: You don’t decide if you have an airway problem that requires surgery based on x-rays. If someone told you based on this x-ray that it might lead to airway problems they are not providing you with proper medical guidance. If you have some form of sleep apnea that you are aware of you get it properly evaluated by a sleep medicine specialist as the first step and get a sleep study to quantify its significance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an existing chin implant but I do not like the effect it has. I am interested to know more about sliding genioplasty and possible some jaw angle implants. I have attached images of what my chin and jaw profile looks like today with the existing implant, and what I would ideally like my results to look like (poorly photoshopped so please forgive me).
My existing implant has brought my chin profile forward a little bit but it has also widened and rounded my jawline from the front and the side. I would like a sliding genioplasty and some jaw angle implants to provide more chin projection, more defined jaw corners, and more of a V shape from the front.
Please let me know what you think and if you need any more information!
Side Note: Patient 27 on your Chin Surgery gallery page seems to have a similar case to mine although I realize every case is unique I believe this is the type of procedure I am looking for?
A: Thank you for your inquiry and sending your pictures. As often happens in a female with a significantly short chin the use of standard chin implants ends up widening/rounding the chin regardless of how much horizontal projection the implant provides. I believe you have come to the more appropriate procedure for you of a sliding genioplasty as you need about 10mm of horizontal chin projection. (+ the current amount of projection your indwelling implant provides…based on your own imaging) But in do doing it will also make the chin more narrow rather than wider. From the side view alone it is hard to draw conclusions about the style of jaw angle implant needed (widening vs lengthening) but that is an issue that will require further imaging from the front and oblique views to ascertain.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Am I a good candidate for rib removal surgery? As you can see in my pictures I am very thin but have no shape.
A:Thank you for your inquiry and sending your picture. Perhaps a surprise to many, the typical rib removal patient looks like you with the identical story…thin female who has maximized their waistline reduction with their own efforts. (diet and exercise) Also interesting they are also the patient that gets the best/most noticeable waist narrowing results.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How can I get rid of this lower fullness in my midface that did not exist prior to a LeFort I osteotomy?
A: In regards to trying to reduce lower midface fullness after a LeFort I osteotomy, a significant maxillary advancement does create a bony shelf that was not there previously. This bony shelf combined with the indwelling hardware can create some projection after surgery that was not present before where the face of the maxilla was concave and now has some bony ledge in the middle of a normally completely concave maxillary surface. In these cases removing the hardware and burring down the bony ledge to recreate a completely concave maxillary surface may help reduce some of the lower midface fullness.
As this relates to you, it can be seen that you have four plates and 16 screws and that your maxillary advancement probably was no greater than 5mms. (as judged by the bend in the lateral plates) This is not the type of maxillary movement that creates a large bony shelf. But it is possible that removing the plates and screws and burring down any existing bony ledge will provide some reduction in your lower midface fullness. But probably going back to exactly what it was before your surgery is not possible as some of the fullness is related to irreversible soft tissue changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m considering face implants with you but I also have thick skin, so not sure if this is the correct procedure for me, fellow researchers have said bimax and other bone cutting surgery’s are more effective in providing a non bloated face. These two people below with thick skin got implants placed and they look bloated instead of angular after, could it be a design issue?
A: In answer to your questions:
1) Let’s first get the concepts correct. A full bloated face is NEVER going to end up with a thin sculpted face…so that end goal should be eliminated as unrealistic.
2) The better question is the how much improvement/slimming effect can be achieved which is a function of tissue stretch (implant augmentation) and tissue reduction. (defatting) The degree of facial change is going to be a function of these combined effects. In the thicker skinned patient both of these diametric tissue changes must be maximized.
3) While I have no idea as to why the implant was designed for the particular patient you have shown, it is an implant design that has its greatest effect in the chin area. The jaw angle portion is so small that it would not have much tissue stretching effect. (But this may be what the patient wanted) It is also unknown what facial defatting procedures were done, if any, for this patient.
4) Orthognathic surgery and custom facial implant augmentations are done for very different reasons. They are not comparative operations and thus their aesthetic effects are going to be different.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is Medpor implant removal more difficult if they are placed long time ago ? Thank you.
A: The time duration of implantation (short of a few days after surgery) does not affect the ‘difficulty’ of Medpor implant removal. I have removed hundreds of them from months to years after they have been placed and the time differences of how long they have been in there does not seem to change how they are removed. In other words, whether it is months or years they offer the same amount of tissue ingrowth. They never get direct bone ingrowth into the material. (some times there is some bone overgrowth but not ingrowth)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I currently have 1350 cc saline implant with internal bra(alloderm)my implant is under the muscle i would like to get around 1800-2000cc and i would like to get a lift too but many doctor have told me that its not worth it if i do a lift because I have a poor skin quality (my skin is too thin and too elastic)and my breast will always get saggy no matter what I do…
Do you think you could help me?
A:An increase in implant volume fights against any lifting effecting effect as well as vice versa. You have to pick one or the other. A lift risks wound dehiscence and poor scarring when done on a very expanded breast skin envelope. It would be more predictable and safer to go with the volume increase only.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Many years ago I had an endoscopic brow lift that left my brows significantly higher than expected, leaving me with what is typically described as a startled, or ‘deer-in-the-headlights’, look. I’m researching as to whether my brows can be lowered and, if so, how much? I have read where, yes, brows can be lowered through reverse brow lift brow surgery, but my case is perhaps more difficult.
Subsequently I underwent FFS (Facial Feminization Surgery). My FFS was somewhat extensive, leaving me to wonder now whether reverse brow lift surgery is even possible.
Besides a brow lift I also had a scalp advancement to bring my hairline forward, rhinoplasty, and supraorbital rims were shaved to reduce brow protuberance. This left me with 2 post-surgical effects I find particularly bothersome:
1. I cannot frown; that is, I have no ‘down’ muscle control. I can raise my brows, but I cannot lower them.
2. I still have a fair degree of numbness in my upper forehead region, extending into my scalp to such an extent that the top of my head feels like I’m wearing a bike helmet.
To both of these concerns I was told by my surgeon that they would self-resolve over a year or so. They did not.
So I leave you with this question: do you believe I’m a candidate for reverse brow lift surgery?
Thanks for your time.
A: Thank you for your inquiry and sending your pictures. Normally a reverse browlift is based on the concept of an epicranial shift…meaning the entire scalp is mobilized and brought forward rather than back as in an endoscopic brow lift. But having had a hairline advancement as well as a browlift (and having lost some forehead skin in the process) would suggest that this approach would not work. You need a more reliable solution to release the scarred tissues AND create more scalp tissue (or at least stretch it better) and that would be a scalp tissue expander. Placed on the back of the head and gradually inflated you would create enough tissue mobilization to get a reverser browlift effect as well as improve the tightness across the top of your head. This would, however, not change the lack of depressor forehead/brow function.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As a child I had an orthodontist to a lot of extensive grinding of my teeth. Later, a car accident damaged my right TMJ joint. Over time, my face has shifted and to the right side. Four years ago I found the best orthodontist in the city and we have worked hard to undo the damage. Now, my bite is repaired and the “melting” right condyle has been stabilized. I am left with the last piece to fix: Correcting my facial tissue asymmetry! I already have a silicone chin implant. I have a large forehead that could balance well with an augmented jaw appearance.
Is there a high risk of the implants failing and has it happened in any of your cases? Is there a risk in my individual case for destabilizing my right TMJ due to the trauma from the pressure and inflammation from the surgery of this implant addition?
Photo Notes:
1)This shows the apparent asymmetry with tissue pulled and favoring the damaged right side. Note this is including recent botox to the masseter muscle with no change in appearance.
2) Please note that the R condyle is practically a toothpick in comparison to the L condyle in the TMJ region.
A:Thank you for your inquiry, sending your picture and detailing your history. In answer to your questions about a custom jawline implant:
1) Failure in any type of facial implant is defined as infection in which the implant needs to be removed. That is about a 5% risk in any standard jaw angle or custom jawline implant.
2) A jawline implant is laid on top of the bone and does not affect its function (opening/closing and chewing) other than during the recovery period from the trauma of surgery.
3) In looking at the panorex (which is a limited 2D assessment) the jawbone has no obvious asymmetry other than the diminutive right condyle.
Dr. Barry Eppley
Indianapolis, Indiana
Dr. Eppley, I have some type of plagiocephaly. The right side of the back of my head is flatter and weirder looking than the other side, and my face bulges out on the right side. I have included pictures, and want to know if its anything severe. What my goal is, is for my head to be how it would’ve looked if I didn’t have the disorder. If being able to make my face look normal is an option that would be of best interest. Thank you so much!
A:Like most plagiocephalic patients the flatter back of the head side is also associated with a right facial protrusion. These are aesthetic issues so the severity of them and the desire to treat them is based solely on how much they bother the patient and what they are willing to go through to correct it. Most plagiocephaly patients that do so focus on augmenting the flatter back of the head and occasionally some reduction of the protruding ipsilateral face. Without a completely straight on facial picture I can not speak as to what may benefit your face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a part time male model considering cheek implants. I have flat cheeks that creates a sad look when not smiling. I’m in my mid forties and have had a mini lift to help improve my mid face and soften my nasal labial folds. It was very helpful, but due to flat checks, I still seem to have what appears to be too much check tissue that lends the sad look. I like the chiseled male model look, in that the cheek bones are more prominent while maintaining a lean area below and do not want a round face associated with most cheek augmentations. It seems most surgeons are focused on submalar implants which does not address my needs which are more prominent bone structure.
Can you share a few before and after pictures of patient to better demonstrate the look that custom implants can produce?
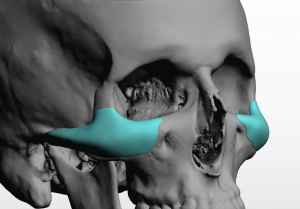 A: Thank you for your inquiry. You are clearly, as most men would, seeking a high cheekbone augmentation look which is not all what standard cheek implants create. This can only be done by a custom cheek implant design which keeps the augmentation located directly along the horizontal zygomatic body-arch line. Whether this would be limited to the zygomatic body-arch skeletal area, which is placed through an intraoral approach, or whether you need a design that incorporates the infraorbital rim (infraorbital-malar style) I can not obviously yet say. For now I will assume it is the former.
A: Thank you for your inquiry. You are clearly, as most men would, seeking a high cheekbone augmentation look which is not all what standard cheek implants create. This can only be done by a custom cheek implant design which keeps the augmentation located directly along the horizontal zygomatic body-arch line. Whether this would be limited to the zygomatic body-arch skeletal area, which is placed through an intraoral approach, or whether you need a design that incorporates the infraorbital rim (infraorbital-malar style) I can not obviously yet say. For now I will assume it is the former.
In regard to before and after pictures almost all of my male patients are extremely private and thus passing around or showing their pictures is prohibited. What few patients have been generous enough to allow their pictures to be shown would be in the website, www.exploreplasticsurgeruy.com searching under Male Custom Cheek Implants and Custom High Cheek Bone Implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a transgender woman, fairly early on in my transition and I am very interested in having the shoulder reduction surgery you offer. I have some questions…
1. How long is the current lead time from booking to surgery?
I would like to try to get the surgery done this year well before Christmas, perhaps early November. Is this realistic?
2. I have previously broken my right clavicle and I think I have a slight deformation in the bone from where it healed (I’ve not included pictures for now as it’s not particularly noticeable but I can of course supply you some if you wish). Could this be a problem? Have you operated successfully on similar patients? I certainly hope it is not a deal-breaker.
3. I will be flying from Finland and then back again when possible. How long will the recovery time in the US be before I can return on the plane?
4. Can you provide a good estimate on the cost?
I hope you can help me! Thank you!
A: Thank you for your thoughtful inquiry in regard to shoulder narrowing surgery to which I can provide the following answers to your questions:
1) My assistant Camille will provide all logistical information in regard to cost and scheduling.
 2) I do not think that a previous well healed clavicle fracture is a contraindication to the surgery. Most clavicle fractures are in the middle and lateral portion of the bone well away from the inner third where the osteotomies are done. (eve if it as in the inner third even better because the healed fracture site would then be cut out) But if you have a post injury x-ray that would be prudent for me to review. I have not yet seen a shoulder narrowing surgery patent that has had a prior clavicle fracture….but it was only a matter of time before that scenario was encountered given the common occurrence of clavicle fractures.
2) I do not think that a previous well healed clavicle fracture is a contraindication to the surgery. Most clavicle fractures are in the middle and lateral portion of the bone well away from the inner third where the osteotomies are done. (eve if it as in the inner third even better because the healed fracture site would then be cut out) But if you have a post injury x-ray that would be prudent for me to review. I have not yet seen a shoulder narrowing surgery patent that has had a prior clavicle fracture….but it was only a matter of time before that scenario was encountered given the common occurrence of clavicle fractures.
3) I have had previous patients from Scandinavia and Europe for shoulder reduction surgery so we are well acquainted with the recovery time for a transatlantic flight to return home. If you are coming by yourself I would plan on a 5 day stay before returning home.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have the same problem your lady seen in pictures has.Case study with the 67 year old female. Does a crooked or larger chin implant make the bunching under chin as seen in picture. My chin looks like this and I have a terrible scar. I have had my chin implant for about 15 years. Just curious as I am doing some research.
Thank you,
A: What you are describing can certainly be due to either an asymmetric or overly large chin implant. But the only way to know for sure is to get a cone beam scan (CBCT scan) so the exact position on the bone and size/style of the chin implant will be precisely known.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Im interested in a rough estimate for infraorbital malar implants AND lateral and supraorbital rim projection to give the appearance of upper midface and masculine dimorphic forward growth with minimal upper eyelid exposure.
Would you advise these put together? would the result look too artificial? Ill be fixing the forward growth in the lower third so I would assume it would look harmonious enough in time.
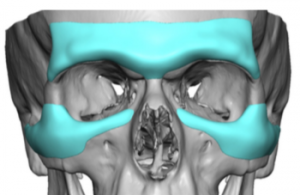 A: As long as both combined periorbital implants (brow bone + inferolateral rim-malar implants) don’t have excessive thicknesses, they should not look unnatural. When periorbital augmentation is performed it is easy to forget the powerful effect of such bony surface area coverage that wraps around the eyes.
A: As long as both combined periorbital implants (brow bone + inferolateral rim-malar implants) don’t have excessive thicknesses, they should not look unnatural. When periorbital augmentation is performed it is easy to forget the powerful effect of such bony surface area coverage that wraps around the eyes.
Whether one does one or both at the same time depends on several factors, most prominently the prolonged appearance recovery that it takes. (4 to 6 weeks)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I may get a hair grafting procedure two months before my custom facial implant surgery with you. Do you have any objections to that?
A: That is really a question for the hair transplant surgeon as to whether this major facial surgery may stress the newly implanted hairs. It would make more sense to me to do it afterwards when a major surgery/anesthesia stressor on the body will be over. It is known that such systemic stressors can adversely affect hair growth or even cause shedding.
Dr. Barry Eppley
Indianapolis, Indiana