Your Questions
Your Questions
Q: Dr. Eppley, My circumcision as a child left me with very little skin on the shaft of my penis, a large amount of scrotal webbing, and a scrotum where it feels like my testicles do not fit. Is surgery and option to reduce the webbing and possibly increase the size of my scrotum so that my testicles sit more comfortably?
A:Penoscrotal webbing can usually be improved by either a z-plasty or a skin graft.
A tight scrotum requires tissue expansion either with a true tissue expander or by the placement of side by side testicle implants to stretch the scrotal tissues.
These are general statements. How they may apply to you requires further information. (pictures that show your concerns)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am a previous patient of Dr Eppley’s, and have an implant across my brow ridge, forehead, and eye sockets. I am interested in getting an eyebrow piercing that would sit over the surface of my implant. Does a piercing in this are pose any risk to the implant, particularly as it relates to a potential infection?
A:It should not as they would have no reason to be down at the bone/implant level with a piercing…..but they should be informed that an implant exists in the area.
Dr. Barry Eppley
World Renowned Plastic Surgeon
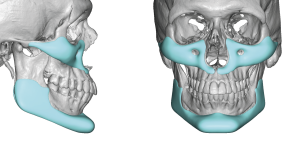
Q: Dr. Eppley, I am interested in a jaw implant to balance my appearance. I am a dentist and before organizing a consultation I could order here a CBCT scan of myself before I go to the US for a consultation with you. Thanks and kind regards.
A:While a 3D CT scan is eventually needed as it serves as the basis on which the implant design is created, it is not essential for a consultation or evaluation…as the scan does not tell us how to make the implant…it is just a platform on which to build it. What is essential initially are facial pictures on which computer imaging is done to determine your aesthetic jaw augmentation goals. That does not need to be done in person which is why most patients anywhere in the world come here only for the surgery. Everything else can be done in a virtual manner.
Dr. Barry Eppley
World Renowned Plastic Surgeon
 Q: Dr. Eppley, Hey how you doing Doc, how you been doing?it’s been a while, I don’t know if you remember Me I was your patient back in 2018 for custom midface and jawline implants. Everything on my side is Great the outcome came out excellent. I have one small thing to ask of you if you could design, it’s something Dental it is called Gingival Mask / gingival Veneers…you see the little problem I still have it’s that the upper gums of mines are still deficient they are flat and by creating this it will add volume by lifting and pushing forward the upper lip area like a Lefort 1 and will also show my upper front teeth. I have created homemade gingival mask but I’m no dentist. the Area of the upper gum I’m talking about are “Alveolar Mucosa and mucogingival junction”… I’ll send you pictures and videos of the gingival mask that I’m talking about, it’s like a denture but for upper gums, it’s actually easy to create but the dentist down here in Florida are just talentless. These are some labs that I’ve read online that dentists send it to create it, Glidewell lab or the Chromeworks Lab Let me know if you could create this for Me thank you.
Q: Dr. Eppley, Hey how you doing Doc, how you been doing?it’s been a while, I don’t know if you remember Me I was your patient back in 2018 for custom midface and jawline implants. Everything on my side is Great the outcome came out excellent. I have one small thing to ask of you if you could design, it’s something Dental it is called Gingival Mask / gingival Veneers…you see the little problem I still have it’s that the upper gums of mines are still deficient they are flat and by creating this it will add volume by lifting and pushing forward the upper lip area like a Lefort 1 and will also show my upper front teeth. I have created homemade gingival mask but I’m no dentist. the Area of the upper gum I’m talking about are “Alveolar Mucosa and mucogingival junction”… I’ll send you pictures and videos of the gingival mask that I’m talking about, it’s like a denture but for upper gums, it’s actually easy to create but the dentist down here in Florida are just talentless. These are some labs that I’ve read online that dentists send it to create it, Glidewell lab or the Chromeworks Lab Let me know if you could create this for Me thank you.
A:Good to hear from you again, I remember you like it was yesterday. Originally being a dentist I am familiar with the Gingival Mask device and as the final piece to your midface horizontal deficiency I can see why that would be appealing to you. This is an acrylic device that is made from an upper dental model that is sent out to a lab like Glidewell as you have mentioned. Since it relies on a maxillary impression/model this is why you should work with a local dentist since this is the foundation on which the appliance is made. Unfortunately you can not use the 3D CT scan from which your midface and jaw implants were made.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Plastic Surgery Case Study – Combining A Custom Jawline Implant with a Sliding Genioplasty This was an interesting article you wrote. Thankyou. Here are my thoughts: I like the idea of a sliding genioplsty (only for the chin) but if resorption of the bone stemming from silicone implants is a primary reason folks go the SG route then doesn’t this approach sort of defeat the purpose? (overlaying to 2 mmm of silicone over a 10 mm SG advancement) or are the forces acting upon the chin different enough in that situation to not be overly concerned? Can you use Peek Custom Jaw Implants that taper down to the chin area for a smooth transition (that covers any step-offs) but doesn’t actually cover the chin in order to avoid resorption concerns on the chin? My other question is do you use custom printed cutting guides and custom built plates to secure the SG? I estimate I need about 5mm horizontal and 5mm vertical but of course, a digital mock up or 3D printed template might lead to a better visualization in order to confirm.
A: I think you missed the main reason a sliding genioplasty is combined with a custom jawline…it is done when the amount of chin augmentation exceeds what the soft chin pad can tolerate. (stretch over an implant) Thus only a sliding genioplasty can be used for the amount of chin augmentation needed.
Can the jawline implant be made of PEEK and can cutting guides be used for the chin….yes on both counts as long as the patient can tolerate the additional costs to do so. And that the use of a very rigid material like PEEK will not permit the jawline implant to fiully merge into the sliding genioplasty. (its rigidity prohibits such placement)
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley I need a revision of my brow bone contouring surgery back in 2014. I would like more information re: brow bone revision contouring while maintaining a male appearance. I have an indentation in the center at the hairline, narrow arched groves from center curving upward & outward toward each side and a small bump on the left side. I see on your website that you have used hydroxyapatite and bone cement for surgical use of brow bone recontouring. I would like to use the most natural product that works with the human body/immune system as apposed to silicone, which the body over time rejects. I would also like to discuss other products, perhaps titanium or other recommendations.
A:The material of choice for any form of brow bone contouring depends on what type of structural change is needed and what type of incisional access is used to do it. Because the brow bone is a small area of the forehead HA can be a good choice as the material demand (volume needed) is low. That being said what is first needed is a 3D CT scan of your forehead to understand the exact condition of the brow bones. I assume you had a bone flap setback in 2014 in which bone defects along the osteotomy line may exist as well as other contour issues as you have described. I would also assume that this was like done from a more wide open access from a scalp incision.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, What kind of scarring can I expect from the surgery?Will this surgery affect a future pregnancy? As in would my rib cage be more vulnerable later on to any kind of breakage or damage while pregnant? I am not pregnant nor plan to be, but wanted to ask.
A:Because this is cartilage scoring and not cartilage excision the two small incisions are each side would be very limited.
No form of rib remodeling has any impact on potential future pregnancies.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I have an asymmetry in my mandible. My left side is narrower then the other side. I came across your website and was wondering how this works for people who live in Europe. Can I send over a CT scan made here for the design of the implant? And can it be send over and do I have to find a plastic surgeon here in Belgium, or is it only possible if I fly over to the US for the surgery?
A: In answer to your custom jawline implant for jaw asymmetry logistical questions:
1) You send me the 3D CT scan (which you get where you liver) from which I design the implant with you in a virtual fashion.
2) You only come here for the actual surgical implantation.
3) You return home in 1 to 2 days and all followups are done virtually
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, My concern is my right jaw as it looks shorter and smaller than my left jaw . My orthodontist said the only way to fix it is surgery or implants but he doesn’t recommend it.Can filler fix this ?
A:Filler may provide some temporary improvement but not a permanent fix. Only a custom implant can provide a permanent fix.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I feel like my face is very asymmetrical and imbalanced and lacks dimension. I feel like I need some sort of implants – cheek or paranasal. And a forehead augmentation – but I don’t know if fat grafting or an implant is more suitable. My right temple goes inward and my right jaw is narrower than the right, so I feel like I need an implant on my right jaw. But at the same time I feel like I need to shave my left jaw and my chin for more contour.
A:While you do have differences between the two sides of your face (see attached grid analysis) when it comes to surgical correction you have to have a very clear idea as to what exact procedures are needed so that the surgical efforts can help minimize the asymmetry. You have described deficiencies which are largely based on your right face which seems correct given that your pictures show a classic right facial vertical asymmetry. (shorter from top to bottom)….provided these pictures have not been reversed. But the first step in facial asymmetry is to get a 3D CT face scan so the bony differences, as most of the facial asymmetry is bony based, can be clearly identified and the properly treatment planned. In most facial asymmetry deficiencies this means custom implant designs.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am reaching out to request a virtual consultation regarding my concerns about the appearance of my forehead and hairline. I have noticed that the prominent bones on my forehead have an unusually large appearance, which has been a source of insecurity for me. I am considering plastic surgery to address this issue and improve my overall facial aesthetics. Additionally, I would like to discuss options for altering my hairline, as it is not as full as I would prefer. After conducting extensive research, I have decided that your expertise aligns with my goals, and I believe that you would be the ideal surgeon to help me. Although I am currently located in the New York City region and unable to travel to your office in Carmel, Indiana, I am eager to move forward with a virtual consultation. I hope that during this meeting, we can discuss my concerns in detail and explore possible solutions. I am looking forward to the possibility of working with you and hopefully proceeding with surgery within this year. Thank you for your time and consideration. I look forward to your response.
A:Thank you for sending all of your pictures. Your forehead concerns represent a considerable challenge for which there is no easy fix. It is a combination of a sloped skull with protruding upper forehead and a significant posterior location of the hairline including the temporal hairline. Each one magnifies the other problem and they are developmentally connected. But it is the hairline that is the worst offender than the bone shape as a more anteriorly located hairline will make the skull-forehead shape look better…but the reverse would not be true.
When considering a frontal hairline advancement the key question is how much forward movement is needed. The reality is that of you don’t get at least 2.5 to 3cms forward movement it would not be worth it. (see attached diagram) This will require a first stage scalp expander to do so.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in your methodology to correct hyperdynamic chin ptosis.
A: You have hyperdynamic chin ptosis because your chin is a bit vertically short which creates a mismatch between the bone and the overlying soft tissue chin pad. This is why the chin pad pulls down with smiling…there is nothing to block it from doing so. Therefore the most effective treatment would be a small chin implant added to the bone to prevent that from happening. This of course will create some modest chin augmentation effect so you have to be certain that is an acceptable tradeoff. (see attached image) The other approach would be a small vertical lengthening bony genioplasty (5mms) done intraorally.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I want to make sure doctor knows about my history . This picture was taking on 2010 and the reason I look good it because I pulled my hair back very tight because not only it pulled my skin but it gives me almond eyes that I truly love but the force of pulling my pony tail so tight it gives me a good look and it made me happy but before pulling my hair tight I used looked like this
It’s a big difference that everyone was shocked . However in 2023 I had my buckcel fat removed so that why I look too hanging checks and also I’m old . I wanted to know in addition to what Dr Eppley wants to do in my face I also was wondering if he can do my eyes in almond shape or Bella eyes this way if my eyes get smaller at least it has a bit of beautiful look I believe that doing my chin as Dr Eppley says and my eyes and Bella eyes than I will have a better sharp eyes.
Bella eyes and also if you look at Maliania Trump. Now she looks like this. So she also shaved her side of her nose and her nose looks slimmer.
A: Bella eyes, or Cat eyes, comes from a combination of temporal lifts with lateral canthoplasties to create that upward sweep to the lateral orbital area. In a young person who has good eyelid skin the lateral canthoplasty is usually sufficient to raise up the outer portion of the lower eyelid. However In the older patient who may have had a lower blepharoplasty with less good quality lower eyelid skin getting a much higher outer position over the eyeball is more challenging and is prone to relapse. This is why a spacer graft is needed in the lower eyelid as well.
When it comes to nose slimming the thickness of the overlying skin plays a major role in how effective that would be. Your nasal skin and Melana Trump’s is quite different as her skin is less thick and thus such structural narrowing changes are going to be more effective. What may also influence the potential change is whether any prior rhinoplasty surgery was ever done. Scarred noses are less responsive than unscarred tissues.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to use a method similar to forehead reduction/facelift to shift down the eyebrows, then use filler in the upper eyelids to create a straight eyebrow and full hooding effect similar to that of Sean O’Pry? When I move the upper half of my forehead down with my hand my eyebrows move to the position I’m looking for them to be in if this helps.
A:First I would be cautious about assuming what you can do with your hand is what can be accomplished surgically….it is often doesn’t work that way. That being said what you are referring to is a revere browlift…releasing the entire scalp and forehead tissues and shifting them downward. While that can be done there are two issues with doing so….1) what is going to hold them there and 2) what is going to prevent relapse with naturally tighter tissues in a young patient. But theoretically that approach would seemingly be effective.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I have glabellar lines that are deep. They currently have a thread(s) and juvederm filler. I was wondering if Dr Eppley would be able to do a permanent filler. I didn’t realize how dangerous regular fillers can be. Also, if so, would you please let me know a ball park cost on this procedure. thank you
A:Permanent fillers do not lower the risks associated with injections into the glabellar area. In fact they increase that risk because of their particulated more occlusive properties.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, inquirimg whether rib breaking or removal surgery would best help correct my flared ribs due to mild pectus excavatum. I have tried bracing, but do not have the discipline to do it for years as instructed in order to fix so exploring other surgical alternatives. Please see my pictures attached for reference.
A:Thank you for sending your pictures which show a lower subcostal rib protrusion. This problem in your case is not best treated by excision but by cutting the cartilages to allow them to bend inward in which a period of postoperative banding (bracing) is needed to help them to reshape. To deter exactly how many of the lower subcostal rubs are involved and where best to place the cartilage scoring a preoperative 3D ribcage is needed for that surgical planning.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a 4 year old son born Jan 2021 who appears to have a “double lip”. He had a tongue and lip tie release at 8 months old in Sep 2021. I am including a zip folder with photos before the surgery and after along with videos to see how his smile was/is.
I need an opinion of someone who is an actual surgeon who understands facial muscles etc and not just a dentist with a knife. Hence why I am hoping you can just tell me if we are making a possible good next move or not. I really value your opinion after seeing some feedback you had previously put online about double lips and understanding the mechanics, cosmetics etc.
After the lip release at 1 year, the lip tigh looks high with a lot of thick tissue. He also has very tight buccal cheek ties that were never released at all. They are hard to picture, but were very thick, low, attaching right above where his teeth meet his gum. He won’t let us pull his cheek open to look so I imagine it is still present.
My concern is his smile now. He has an apparent crease across his upper lip when he smiles. It’s not obvious at all when resting – the smiling “big” creates it. The crease runs the full length of his upper lip. Is this a double lip? I’ve read that can be caused by trauma – did the release cause this? Double lips usually involve removing the redundant tissue but that would leave him with barely any upper lip. I can’t tell if the “double lip area” is outer or inner lip tissue that should even be resected. Before surgery, when smiling, did he have much of an upper lip? It was almost cliff-like if that makes any sense.
We are now faced with what to do next. We are exploring the option to re-release what’s left of his upper lip tie, and maybe ask for the buccal ties to be released too. With your knowledge of anatomy and the cosmetic side of things, would this potentially resolve the distortion in his upper lip? Or could it release the tension (particularly if the buccal is still strong + reattached upper lip).
We are beside ourselves wondering what the right thing is to do. I really appreciate anything you can offer.
A:Unless the upper double lip is causing a functional problem, which I am sure it isn’t, you need to leave it alone for now in a young growing child. I am not sure this was not caused by the maxillary frenulectomy…of which what the compelling need to do so was at such a young age. The upper lip may or may not have been caiued by the frenulectomy. This may be the ‘rabbit hole’ effect…you do one thing to fix one problem and then you develop a new problem. The goal is to get out of that cycle which in surgery is easy….stop doing surgery unless there is a compelling medical need to do so.
Double lip correction is an effective and straight forward procedure and can be done at any time. But I would let him grow some more and let his facial tissues develop further. I would only correct the double lip or any of the other associated issues when he is older and he finds it to be an issue.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley ,I have searched all over for assistance with a lower rib on the right side of my body. It cracked in year 2020 with a fall, when it healed I was told it over produced the bone substance used for healing the cracked rib. This has caused me to have severe discomfort as it feel like I am being stabbed from the inside out. At one point they did an exploratory surgery to determine it was in fact my rib. I have been to: 2-3 PCP, an orthopedic surgeon, a neurologist ( thinking numbing nerves would help ). I am out of options, everyone tells me I am stuck with this. I can’t workout anymore, run and jump as it pokes me, sex is hard. It is really killing my quality of life and depressing me. I would like to see about fixing it, as it’s causing pain. Yes, some days are worse than others. I can’t even sit at times. I have been googling things and your practice came up, is this something you would be interested in looking into for me? I have read it may have to be out of pocket, but I have also read since it’s related to a past injury and causing pain we can work in insurance as well. Please help
A:I assume the exact rib is known and there is an x-ray (plain film) that shows its location. (need that info) Rib resection would be the logical treatment approach. The only question is where it is located and can it be safely reached.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley,I am inquiring about a sliding genioplasty. I have attached some photos to show what would roughly be my goal in this surgery. My chin is recessed and seems that it would require some downward and forward repositioning to achieve a desired result. I was wondering if this seems within reach with this type of surgery.
A:I don’t think that type of chin augmentation change is completely achievable. What you are showing is a significant horizonal advancement and significant vertical shortening….a change only remotely possiboe with a sliding bony genioplasty., The problem is that with a conventional sliding genioplasty it would be very challenging and almost impossible to get that amount of vertical chin shortening no matter how much you tilted up tehg repositioned chin bone. Such a change requires a jumping genioplasty where the cut chin bone is moved directly in front of or ‘jumped onto the bone above it. The problem with the jumping genioplasty technique is that you never know whether the attached muscles to the down fractured chin segment will allow that amount of stretch to make that jump….sometimes it will and others it may not in my experience.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, “Hello I read online you can reduce the width of the hips/iliac crest.I need some information, i am from the Netherlands but did not founded anyone here how does this surgerywhat are the disadvantages? Can complaints arise after the surgery?”
A: You are referring to iliac crest reduction which. is associated very issues if any other than the small incision/scar needed to do so. The most important issue is whether the procedure would be effective for your goals. I would need some hip pictures to do some imaging of potential results.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, do you offer a service to design a chin/jaw implant only from a supplied CT scan or solid model of the Mandible (pre-segmented). The design would be used to print in PEEK for use by another doctor/patient outside the USA. Thanks
A: I do not design implants for other surgeons to place.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Can my visible temporal arteries be ligated? I have attached pictures.
A: These are classic prominent temporal arterial branches that are takeoffs of the main temporal artery. (not the more common anterior branch of the superficial temporal artery) But regardless of this anatomic variation they can be successfully ligated.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I hope this email finds you well. I would like to inquire about treatment options for plagiocephaly. Specifically, I have noticed that the left side of my face is more protruding compared to the right, with a tilt to the right as well. I wanted to ask if it is possible to address this asymmetry through cheekbone reduction and shaving, particularly the anterior zygomatic prominence, as it appears longer on the affected side. Additionally, I would like to know if anything can be done to address the protrusion of the eye on the same side. Furthermore, I have noticed that the skin over the ear (I believe it is related to the masseter muscle) appears baggy or “puffy.” Is there any way this can be stretched or addressed without a skull implant? Otoplasty and a orthognathic surgery is something I’ll definitely check to. Thank you for your time and expertise. I look forward to hearing your thoughts.
A: When it comes to reductive facial asymmetry corrections there are a variety of bone reduction techniques of either osteotomy or ostectomy. (shaving) How effective they would be requires a 3D CT craniofacial scan to assess the bone differences and thicknesses on the larger asymmetric side. That is where to begin the facial asymmetry surgery process.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I am interested in this technique for its potential to improve scalp hair growth, I shaved my head once and I realised that I have quite an odd shaped head, and I also read that perhaps skull shape, effects hair growth. I guess through restricting or liberating blood flow to the follicles.
A: Having performed over 500 skull implant cases I can’t say any patient has reported after surgery that they noticed increased hair growth. In theory the placement of s skull implant does block vascular ingrowth from the bone or fascia over which it lies. To maintain scalp vascular homeostasis blood must be increased through peripheral channels to the expanded scalp. While it is tempting to think that this vascular change can stimulate the hair follicles I have not conclusively seen it. While I wish that was true the proven benefits of skull implants are for contour change.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, Hello I’m looking to get a custom jaw implant later this year. Do you have any specific information about the procedure and recovery that might help me make a decision about choosing you as my doctor? I will be coming from New Mexico and will be alone. Will I need someone to take me back to my hotel after the surgery or is there something else you can provide? Thank you
A: Having performed over 500 custom jawline implant surgeries and having written about this topic extensovely I would refer you to the following three websites which provides a wealth of information about the procedure.
www.exploreplasticsurgery.com indications, surgical technique, implant designs, recovery
www.eppleycustomfacialimplants.com implant designs
www.eppleyplasticsurgery.com before and after patient photos
Having an international practice where most patients fly in from all over the world for surgery, and most are traveling alone, we are well versed in managing the logistics of the surgery from arrival to departure.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, What materials available for implants? I see he uses a lot of silicone and was wondering why that is. I prefer different material would that be okay?
A: There are a variety of materials for custom facial implants including solid silicone, Omnipore/Medpor, PEEK, PEKK and titanium…each with their own advantages and disadvantages There is no perfect faciak implant material.
While patients and even most surgeons get caught up in the implant material properties on a handling basis, often with very erroneous perceptions in vivo, to the body an implant is an implant is an implant. It is still a foreign material and no material offers any different or superior biologic benefit.
What separates these facial implant materials is not their biologic responsesbut other features such as cost, design limitations, and ease of placement and revision/removal .
Given that the revision rate of any custom facial implant is in the 40% range (shocking to patients but true), the concept of ‘easy in, easy out and easy back in’ has great clinical merit. This is where solid silicone has a significant material benefit and explains its broader clinical use than the other materials.
That being said it does not matter to me what material a patient wants to use as I have placed and removed every implant material that is available. What I care about is that the patient understands the advantages and disadvantages of their material choice.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in feminization surgeries. I currently present male, and would like to do surgeries before moving on. Ultimately I would like to have a number of procedures, but have no idea about cost or insurance. I had gastric sleeve performed 18 months ago and have lost 100 lbs. 5′ 9″ currently 180 up from a low of 170lbs. 48 years old next month. Procedures i am interested in: Butt and hip augmentation. (Currently thinking solid implants are preferable to fat grafting) Floating rib removal and/or repositioning Mid rib(lower attached ribs) repositioning Clavicle reduction Liposuction. (Belly, upper/lower back, thigh..etc) Overall skin removal and tightening (belly, butt, thighs, lower, mid and upper back) I am willing and able to travel for procedures and recovery. I would really like to get info on which procedures can be done simultaneously and approximate cost. Would like complete as much at one time as possible. Would also be interested in FFS at a future time. Thank you
A: When it comes to body feminizing surgery you have one unique anatomic feature that separates you from most other patients…..the large amount of weight loss. (massive weight loss or MWL) This creates the need for numerous body contouring procedures (skin removal and tightening) that do not necessarily have feminizing effects but are more of a ‘reconstructive’ nature. As a result considerable thought must begin to both MWL and body feminizing procedures to create a staged surgical plan for maximum efficiency and effectiveness.
That process begins by looking at your body pictures from numerous angles (front, back and sides) for an initial assessment.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I am interested in replacing my PEEK infraorbital-malar implants as they don’t saddle the rim and as a result they stick put unnaturally. These implants were placed intraorally at the time of double jaw surgery.
A: Be aware of two very relevant aesthetic issues. 1) when have to saddle the infraorbital rim you have to use a lower eyelid incision to do the dissection needed as well as to ensure proper placement and 2) PEEK is not a good implant material for thin tissues like the lower eyelid and orbital rims as it can not be made withj feather edging as it is machined in its fabrication. You will likely end up with visible edging even if it saddles the rim. …less than what you have now just at a different level and degree
There is a reason your current PEEK implants don’t haver a feathered edge design and look bulky…which is very obvious in bot the design and after actual placement. This is a design limitation of all very rigid materials that have to be machined in manufacturing. There is always going to be at least a 1mm edge. This is not an aesthetic issue in thicker tissues like the jawline and lower cheeks. But it will be one around the orbital rim which is an unforgiving implant placement site.
Dr. Barry Eppley
World Renowned Plastic Surgeon
Q: Dr. Eppley, I have a separate medical enquiry, regarding bone burring to correct the prominence of my forehead. Can this be done please. Not sure if I’m imagining things but my right side seems to appear a bit smoother than the left, so it’s this left side I would’ve wanted addressing.
A:Are you referring to the prominence of your forehead or that of the brow bones. I ask because I don’t see any true forehead prominence. The other issue is for any forehead work where is the scalp incision going to be placed to do it. In the male with short hair here is no aesthetically hidden place to put it.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley I hope this email finds you well. I’m reaching out to ask about surgery for the two horns on my forehead that stick out noticeably. I’ve attached a recent photo to show how they usually look.
I have a few questions:
1. How is the procedure done?
2. How much does it typically cost?
3. Will I be able to safely play soccer afterward, especially since I frequently head the ball?
I’d appreciate any details you can provide and look forward to your guidance.
Thank you for your time and expertise.
A:Forehead Horn reduction is typically done by bone shaving through a small scalp incision. In very large forehead horns like yours the key question is whether the bone is thick enough in the horn area to permit an adequate reduction. This requires a CT scan to make that assessment. Provided reduction can be safely done there would be no postoperative limitations in terms of playing soccer or any other activity where trauma to the head can occur.
The CT scan can be done in our local area and we provide the order form at a local imaging facility to have it done.
Dr. Barry Eppley
World-Renowned Plastic Surgeon