Your Questions
Your Questions
Q: Dr. Eppley, I like your explanation about Brow Bone Hypoplasia on website and I am thinking get this done, I am asian and I like the asian model’s result on that section, my purpose to have brow bone raised to have more eye depth and more defined look.
I do have couple questions if you don’t mind, where and how long is the incision for PMMA or HA on brow bone? in the hair? so the forehead skin would be opened to reach the brow bone right? I know Radiesse is calcium hydroxyapatite (CaHA) gel microspheres filler , can we reach the same result using Radiesse filler , multiple times of injection of course since most of it dissolves . lastly, 3D, you meant 3D printing right? what material do you use for that? is there a risk of implant movement in normal daily activities or exercises?
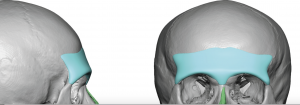 A: Thank you for your inquiry. Permanent brow bone augmentation is done best by a custom brow bone implant, not injectable fillers or any form of bone cements. These require big incisions to place (bone cements) and are unreliable in shape. Custom brow bone implants are placed through small incisions using an endoscopic technique. Being preformed by computer design they have a reliable shape and can be properly placed to provide the soft tissue push to create the desired aesthetic effect. Once these implants are in position and secured they will never move despite what one’s daily activities or exercise regimen is.
A: Thank you for your inquiry. Permanent brow bone augmentation is done best by a custom brow bone implant, not injectable fillers or any form of bone cements. These require big incisions to place (bone cements) and are unreliable in shape. Custom brow bone implants are placed through small incisions using an endoscopic technique. Being preformed by computer design they have a reliable shape and can be properly placed to provide the soft tissue push to create the desired aesthetic effect. Once these implants are in position and secured they will never move despite what one’s daily activities or exercise regimen is.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,After a few months of thinking about this I think I want to reinsert fat back into my buccal area. Just not satisfied with the look, my face just looks too skinny. I probably just should’ve went with the buccinator myectomy and perioral mound liposuction initially cant change the past and can only move forward. My question is what would be the price to reinsert fat back into the Buccal area and was it documented the amount of cc in fat that was removed to fill the area back up properly? Thanks
A: There are two ways to restore buccal fad pad volume which is in the 2cc to 3cc range, fat injections or the insertion of en bloc (solid) fat graft back into the buccal fat pad space. Each method has its advantages and disadvantages. Usually the latter is more effective as it puts the volume directly back into where it was initially removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I only need a change my nose, a rhinoplasty revision. There is implant in my nasal bridge. My nose was very flat before the implant. What I need now is reduction the tip of nose and a symmetric nose. Is that possible?
A: Thank you for your inquiry and sending your picture. While obviously I have no idea what was done actually in your rhinoplasty (other than some type of implant was placed) I don’t yet have enough information to determine what type of nasal improvements can be done. To provide a qualified answer to that question I would the following two pieces of information: 1) a front view picture and 2) a copy of the operative note from your prior surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is ” Cool Sculpting ” an effective method of permanently reducing fat from underneath the chin? (double chin)
A: From an ROI (return on investment) standpoint…no. Surgery is far more effective. Such technologies exist for those patients who are willing to go to great lengths to avoid surgery…and are willing to accept a very modest non-surgical type of result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I was wondering whether you can return back to a contact sport like boxing after temporal muscle reduction and if so how long is it you have to rest.
A: You should be able to return to contact sports within 30 days or less after temporal reduction surgery. Since tissue is being removed you can not hurt the surgical result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been thinking about getting this looked at for some time. I am missing a tiny bit of bone in my brow bone just under my left eyebrow causing my eye to move freely within its socket (vertical orbital dystopia) as well as having a prominent left brow and what I’d like to do is get an MRI or anything to figure out what I could do to achieve symmetry within my face.
A: I think your right vertical orbital dystopia (VOD) is really part of an overall right facial hypoplasia. But the first place to start is to to get 3D CT scan of your face which will clearly show the location and extent of the right facial bone differences from that of the left side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a quick question for you, can you suggest a surgery to define my jawline (picture 1) so it looks like picture 2?
I noticed that when I tighten the skin around my jaw, like picture 2, I get the desired effect on my side. I have already a strong jawline by nature ( picture 3) but its not showing on the sides for some reason. Could you help with this in your practice?
A: What you are doing by biting down is flexing your masseter muscle creating a jaw angle enhancement of increased width. This is a pure lateral ramus augmentation which should be achievable by placement of an implant underneath the main section of this muscular region. How much implant width is needed to create that effect is speculative but I would estimate between 10 to 12mms per side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently interested in Lip Reduction. Based on my research, it appears that you have extensive knowledge in this procedure, so I just wanted to ask for your opinion so that I’m better informed.
I had a Lip Reduction procedure done almost 6 months ago and noticed almost no difference, except at the far left/right sides. I believe this may be because my doctor only removed tissue from the wet mucosa region. In fact, when I look at the scar in my lower lip, there is wet tissue on both side of the scar. From what I’ve read in your blogs it appears that the correct approach to Lip Reduction is to remove some amount of dry and wet vermillion? Or is the correct approach only to remove dry vermillion up to the wet/dry border? Why do you think so many doctors incorrectly remove tissue in the wet mucosa region only? Thanks for your opinion, I appreciate it! For reference I’ve attach a before and after photo.
A: I can not speak for what other surgeons do or what your surgeon may have done in regards to the approach to lip reduction surgery. But I have learned that effective lip reductions come from removing the more exposed dry vermilion, which is more effective at rolling back the exposed vermilion height. (which is how lip size is perceived) The wet mucosa is very mobile and will have little effect on reducing the exposed dry vermilion. I suspect that placing the scar line in a potentially more visible location is a more risky proposition to some surgeons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My aesthetic concern is that when i look down my jawline disappears and i have a double chin, even from a raised head I have a slight wobbly double chin despite being like 145 5’10”.
I was wondering if off the shelf implants would work because I do not need to look like a movie villian, though I’d like to go for as dramatic off the shelf implants as available.
A: The difference between custom vs standard chin/jawline implants is not that one creates a more dramatic effect than the other one. It is more about controlling the implant design/dimensions before surgery and making the implant to specifically fit the patient’s anatomy. This potentially lowers the risk of certain aesthetic complications.
That being said in lieu of a custom jawline implant the other options are a standard chin/sliding geniopasty with standard jaw angle implants. Given your chin recession and the submental fullness a sliding genioplasty would be more effective at resolving these issues than a chin implant because of the forward pull of the chin bone on the submental musculature.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have inherited weak cheekbones from my father that have resulted in both under eye circles from the lack of cheek support and an overall very flat profile. It makes me look tired and even ill, but no weight gain can impact that area of my face. I would much rather have full, feminine cheeks with a visible curve.
1. Is this possible to achieve through standard implants or are custom ones necessary? Can you place tear trough implants and combined submalar shell implants at the same time?
A: It is never a question of whether a custom infraorbital-malar implant design is the superior approach for the complex topograpy of the eye-cheek area…because it always is. You only choose the old style approach of combining standard tear trough and cheek implants for pure economics reasons with the understanding that an inferior aesthetic outcome is better than none at all.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had a lip lift (about a month ago). The Dr. was a renowned and qualified surgeon who had excellent reviews and is considered one of the best at lip lifts. I only wanted a few millimeters off. about 3 mms. Despite my request he ended up taking off “half my lip” as he said or over 8 mms. I now have an A frame deformity. My mouth is constantly gaping open. I read your website about avoiding this. Is there anything that can be done to fix this? I’m heartbroken and in shock and depression. I also wonder if other places have a formal way of agreeing on pre-op plan in writing? Because there was no formal written agreement there was obvious miscommunication. I’m wondering if it is normal for this big of a procedure to just be verbal consent and no formal surgical plan or blue print, so to speak. Any help or advice you can give would be greatly appreciated.
A: One of the fundamental principles of all surgical lip lifts and advancements is that they irreversible. Once the skin is removed there is no putting it back. Subnasal lip lifts do relax/settle/drop down to some degree up to six months after the procedure. That is usually but a millimeter or two. So all you can do is give it time and see how much, if any, dropping of the central upper lip occurs.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have hip implants but they don’t look natural. You can see the contour of the entire perimeter of the implants. I have had them revised and the revision did not conceal the edges of the implants. Two questions:
1. Could sculptra be used to surround the hip implants and soften their edges so that my curves are nice and smooth?
2. Could fat injections or flap surgery be used to cover the hip implants and soften their edges so that my curves are nice and smooth?
Looking forward to your feedback.
A: You have three options to treat hip implant edging. 1) Injectable filler or fat injections, 2) reposition the implant under the capsule that currently exists (improved soft tissue cover) or 3) improve the edge shape of the implant. (some implants do not have a true beveled feathered edge) Since I don’t know what hip implants were used in you I can say how that would apply to you. In my experience #2 alone possibly combined with a better implant shape usually improves/solves the problem.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, I’m 25 year old I’ve having similar skull issues as attached, Is it possible to be reshaped kindly advise.
Q: Dr. Eppley, I’m 25 year old I’ve having similar skull issues as attached, Is it possible to be reshaped kindly advise.
A: Plagiocephaly is one of the most common reasons people present for skull reshaping surgery. Whether it is the back of the head and/or the forehead both skull regions can be reshaped.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a cranioplasty surgery done over 15 years ago which filled in my large brow bone and dents in my forehead. We did an MRI of my skull. He cut me from ear to ear and went that far with the cranioplast. The problem is that he did not raise the top of my head. My head looks very flat and slopes down to the back of my head. I wanted to know if I could get a custom implant to fit along with the cranioplast and raise the top of my head. I can sent a picture of what I am referring to.
A: Thank you for your inquiry and sending your pictures. Certainly a custom skull implant can be designed to raise the top of the head and otherwise create an overall head shape that matches better with the prior anterior cranioplasty procedure. The 3D CT scan will clearly show the PMMA material of the forehead and brow bone areas from which the design of an implant to create the desired changes to the rest of the skull can be done. The existing scalp scar provides a convenient point of access to place the implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, At birth they pulled my head so hard my skull really stretched out. I camouflage it well with my hair but its still bothers me. Are there any possibilities for Total skull replacement with custom implant?
A: While you can replace your skull bone with an implant, that will not be of any benefit since you can’t squeeze it down or make it smaller because of the brain which has expanded to fill that space that the skull shape has created.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have lip incompetence/mentalis strain. I have tried relaxing with Botox and it had worked but it is not permanent. I have been to the orthodontist and I have a slight skeletal open bite for which they said only jaw surgery would be able to fix my incompetent lips. However jaw surgery is a very risky and expensive procedure and I do not want to go through with it. Can a sliding genioplasty be able to bring the chin in a more forward manner and reduce the strain/incompetent lips? Thank you!
A: Improvement in lip competence and reduction of mentalis strain in some sliding genioplasty patients is one of the potential benefits of the surgery. But that would depend on what type of chin movements are done and what is the anatomy of the patient’s chin initially.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a sliding genioplasty five years ago and hydroxyapatite paste added to the jaw angles. However, the HA paste is VERY uneven and one side is rounded and the other more angular. I tried to have it removed but the surgeon was unable to remove it since it had integrated too much into my tissues. Could a small amount of HA paste be added to even it out? Ive tried fillers like Juvederm and Volux (designed for chin and jaw augmentation) and Radiesse in the past but they are still too soft to emulate bone and end up looking puffy after a few weeks.
A: You have encountered exactly what one would expect with using HA paste in the jaw angle areas…asymmetry and irregularities. It is hard enough to place preformed implants into the correct position over the jaw angle area let alone an amorphous paste.
I am not sure why the combined material/bone can not be removed despite having some bony integration which is exactly what one would expect to happen in a subperiosteal pocket with a thick overlying muscle layer. (it is a highly osteogenic site) It is not easy but that should not be confused with can’t be done. But that issue aside secondary HA augmentation can be done. The relevant question is how much volume and where should it go….an imprecise secondary procedure for sure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have Poland’s Syndrome. Do you offer custom pec implants or are they pre-made?
A: All Poland’s syndome pectoral implants are custom made. It would be impossible to achieve a good result in most cases with a standard pectoral implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was affected by positional plagiocephaly after birth and now have a strange head shape. Can total correction of the skull be done in heads like mine which would include the forehead, temporal and back of head areas?
A: Optimal treatment of cranioscoliosis from positional plagiocephaly would involve the forehead/frontal (reduction vs augmentation), temporal reduction and back of head augmentation. The question is not whether that can be done but whether all mentioned skull regions need to be treated and whether the various incisions needed to do it (particularly the forehead/frontal region) are worthy tradeoffs for the benefits. That would have to be determined on an individual basis.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a slightly recessed chin. I want it to be more protruded and shorter. My profile angle is also weak (is there an alternative to getting implants? can bone be broken instead to wake it wider?)
My cheekbone is also flat on the front view. I’ve had a previous consultation, the doctor said that my cheek is quite low for my age. I just want it to be more lifted and to have more angle. But the side view of my cheeks is alright for me and don’t want it to be more apparent. Only on the front view.
i sent a pic of me smiling. i don’t like it when my cheeks elongate, they look like chipmunk cheeks….I recently had a buccal fat removal to see if it could improve my face. i would not like an implant to make them bigger…so just want a more structured and defined cheeks.
A: In answer to your questions:
1) The pnly chin option to make it longer and shorter is a vertically shortening sliding genioplasty.
2) Jaw angle augmentation can only be done with implants. No bony method can ever make the jaw angles wider or more pronounced.
3) With a flatter cheekbone on one side the options are either a small implant or fat injections.
4) There is no surgery that can change the way the cheeks look when you smile. You have probably learned this from the buccal fat removal. Smiling is a dynamic maneuver while surgery only affects structures in their static position.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read your comparison on medpor and silicone jaw and chin implants, you say that there is some bone erosion that happens after placing implant.
My question is will chewing gum (flexing jaw muscles) and moving chin muscles result in more bone erosion than it would be if one never chew any gum, in both silicone and medpor implants (does chewing gum has impact on bone erosion after placing implant)?
Also you say there is soft tissue ingrowth in medpor implants, did you meant jaw muscles?
Thank you!
A: In answer to your questions:
1) Bone imprinting occurs with all facial implants, regardless of its material composition. It is a natural biologic reaction.
2) Such bone imprinting is not affected by motion or overlying muscle pull.
3) Fibrous soft tissue ingrowth occurs on the surface of any textured or porous implant material.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in hip pelvic implants but not the kind that are simply stuffed into a pocket, I’ve been to numerous doctors and the only type of procedure they do are standard hip implants stuffed in a pocket. I have contacted a hospital in Seoul that is known for pelvic plasty but noticed one of your replies on Real Self in response to a similar inquiry. I am very lean and narrow hips and are looking to round out my figure. I am also a trans woman which only adds to my hip deficiencies. I have attached photos for your review. Look forward to hearing back from you! Thanks so much!

 A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. (see attached) As you know only the country of Korea offers such implants made of metal…which may (or may not) be the ideal material for augmenting the iliac crest. No one really knows since so few such surgeries have ever been done. Here is the U.S. metal iliac crests are not an FDA approved device. (and may likely never be approved as a cosmetic implant given the low demand for it) No U.S. orthopedic manufacturer will even make it as a custom implant because it falls outside of their FDA reconstructive implant approvals. As a result I have designed ultrafirm solid silicone iliac crest implants as an option here in the States but have yet to actually implant them in a patient to date.
A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. (see attached) As you know only the country of Korea offers such implants made of metal…which may (or may not) be the ideal material for augmenting the iliac crest. No one really knows since so few such surgeries have ever been done. Here is the U.S. metal iliac crests are not an FDA approved device. (and may likely never be approved as a cosmetic implant given the low demand for it) No U.S. orthopedic manufacturer will even make it as a custom implant because it falls outside of their FDA reconstructive implant approvals. As a result I have designed ultrafirm solid silicone iliac crest implants as an option here in the States but have yet to actually implant them in a patient to date.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As you can see from the photos I suspect a webbed neck deformity (pterygium colli). I have already done the Noonan syndrome’s genetic test and it’s result was negative. I would like to know if i could be operated to correct this deformity and what should i do. I wait for your news.
A: Thank you for your inquiry and sending your pictures. Webbed neck surgery is based on excision of tissue on the back of the neck. Its success depends on how much laxity of the tissues exist as well as the acceptance of a midline scar on the neck.
That being said, you have two issues of concern for his surgery. First you are a male with shorter hair where the resultant scar will be exposed. Having never yet having a male request or undergo the procedure I would have concerns about the appearance of the scar in a more exposed area. (in women with longer hair this is not a concern) Secondly, intermediate neck webbing like yours is associated with tighter tissues that often resist or have greater amounts of postoperative recoil to the midline pull of the procedure.
This is not to say you can not undergo the procedure successfully, these are just preoperative issues to consider.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, With vertical orbital dystopia, is it possible to lower the eye that is situated higher if one prefers the appearance of the lower eye/mid face or is such an approach impossible? The infraorbital bone would have to be shaved down I assume but placing an implant superiorly above the globe would probably involve greater health risks. Are nerve damage and vision problems likely complications with these kinds of procedures? I suspect my dystopia would be in the 5mm range. It really ruins facial harmony and I noticed people that are widely considered attractive almost always have either none or very little eye asymmetry. Is it possible to receive a quote for a possible surgery assuming it would involve cheek and eyelid work as well? (the sides of my face are asymmetrical across the entire face)
A: To lower a higher eye that is done by dropping down the bony orbital floor like is done in orbital decompression surgery. This is not a precision procedure, like raising the eye with a premade implant, so exact amounts of lowering are hard to predict. Besides that issue the more pertinent concern is that the position of the upper eyelid will remain the same when the eyeball lowers…affecting the lid-globe relationship. Unlike raising the eye where the upper eyelid can be surgically raised by ptosis type procedures to restore the lid-globe relationship, there is no surgical procedure to lower an upper eyelid. Thus another aesthetic problem may result with too much scleral show between the upper eyelid margin and the superior margin of the iris.
I would need to see a picture of your eye asymmetry to determine how these potential issues may apply to you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was interested in receiving more information on the Occipital knob reduction. In addition how safe is having this procedure completed? I am apprehensive due to concerns of safety and anxiety considering I have never had any other surgery.
A: Occipital knob skull reduction is a perfectly safe and effective surgery. The occipital bone is thickest of the skull bone particularly along the nuchal ridge area so the brain is safely removed from the reduction area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I just recently found out through your blog that as a child I had positional plagiocephaly. I have a flat spot on the right side of the back of my head. I have always thought there was something wrong with my eyes and was in the process of finding a surgeon for my facial asymmetry. I now know where the asymmetry came from and I really want some of the asymmetry to be improved as much as it came be. I personally like my right eye better because it appears bigger and more of the eyelid can be seen. I also believe I have a small deviated septum which causes my nose to curve over to the right which I would prefer be fixed If I do a consultation will it need to be done in person due to the cause? I’m not sure what needs to be done to make my face feel more symmetrical so I am hoping your practice can help me. Thank you so much!
A: Thank you for your inquiry and sending your pictures. Your facial asymmetry is undoubtably due to congenital plagiocephaly. The left eye is more posteriorly positioned as is the brow bone, cheekbone, and infraorbital rim. The challenge in preferring the right eye is how to make the left eye appear more similar. One thing you can not do with an eye is to bring it further forward since it is attached/tethered by the optic nerve. Thus the left eye can not be brought further forward which is the ideal manuever to improve the eye symmetry. But besides being more posteriorly positioned it also sits a bit higher. The orbital floor can be lowered which will being the eye down a bit. That combined with cheekbone reduction should help the eye/facial asymmetry.
A 3D CT scan of the face is the first place to start in making an accurate assessment of the bony asymmetries and in making a more informed treatment plan for them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My lower face is much wider than my forehead. Getting older has accentuated this effect. I have just retired this month and would like to go into my later years looking a bit less cartoonlike. Would prefer to under-correct than overcorrect, however.
A: Thank you for your inquiry and sending your picture. Aging has increased the wider lower facial appearance with the typical soft tissue descent that occurs. The soft tissue can be relocated/resuspended by a neck-jowl tuckup procedure which is the basic approach that is needed.
The more pertinent question is since this is a natural/congenital issue there is a bony component to the lower facial width as well as a naturally more narrow forehead. In treating this issue more comprehensively at the bone level the options are for a jaw width reduction or a forehead augmentation/widening procedure. There are advantages and disadvantages with either approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! My frontal bumps are very pronounced and I want to get rid of them, but my hair is not thick and I’m balding, so I can’t do surgery with a coronal or hairline incisions, a big scar is not acceptable for me.Can I reduce the frontal eminences endoscopically? One doctor said that endoscopic removal is dangerous, why? If an endoscopic osteoma can be removed, then why can’t the eminences be removed as well?
A: An endoscopic technique is not going to work for frontal eminence reductions because such reductions require power equipment which can not pass through a small incision or work around a curved surface. Frontal eminences are broad based bone elevations of the outer cranial surface.
Conversely endoscopic removal of osteoma uses an osteotome which is effective for them because they are bone growths just above the outer cranial surface that is attached to it by a narrow base. (like a mushroom) Thus they are rather easily separated from the surface by the osteotome.
The one intermediate technique that I have found useful in cases like yours is the rasp technique. With incisions as small as that used for endoscopic surgery a large toothed rasp is inserted which can aggressively remove bone manually. It is a blind technique where the reduction is ultimately guided by eternal appearance and feel.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is 3cms of lengthening on each clavicle possible? Im 6’3″ tall and very narrow and hope for the best possible result.
A: Thank you for sending your picture. It is also a balance between how much clavicle lengthening can be achieved vs ensuring that the bone will heal properly. The longer the lengthening the better the aesthetic result but the higher the risk of non-union. I would agree that 3cm of lengthening per side would be best but until I get to surgery and make the bone cuts I can not say whether that length is achievable.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What do you think about using long term resorbable meshes for augmentation of flat back head? I have such a condition and I saw a plastic surgeon conducting augmentation using non-absorbable meshes. I would not like to have foreign material in my body for ever but I am really curious about resorbable meshes and their effects in cranioplasty.
A: I could not imagine that a non-resorbable or resorbable meshes would be a very good skull augmentation material for a variety of reasons. Perhaps for very small amounts of ‘spot’ augmentations it may be fine but for the much more common larger surface area skull augmentations that most people desire it would be a far inferior material choice. The key criteria for an aesthetic onlay skull augmentation material is: 1) having a smooth outer surface contour and fine feather edges, 2) easily modified or removed later if the patient is unhappy with the result or desires a change, and 3) able to be placed and properly positioned through small scalp incisions.
There is a corollary to your question and that is the use of mersilene mesh for the chin …which has never become a mainstream technique in chin augmentation surgery.
Lastly non-resorbable meshes are synthetic polymers…an implant material in the skull that may never really absorb. It has never been tested for that implantation site. One should not confuse what happens when such a material is implanted on muscle vs on top of skull bone.
Dr. Barry Eppley
Indianapolis, Indiana