Your Questions
Your Questions
Q: Dr. Eppley, I have a question about extra-oral placement of a vertical jaw lengthening implant and infection rates. I had a 7mm width jaw angle implant placed, which for my extremely short/stocky face with almost no ramus/mandibular distance from the earlobe made my face puffy and squirl like (i am a male). It got worse because my jaw joints over time degenerated and moved even more backwards and vertically, to the point I will be needing a total jaw joint replacement and removal of the jaw implants. My question is: is it possible to have a vertical lengthening implant after the jaw joint replacement. In theory in the pictures it looked like it should be possible, but the lack of room for screw placement is what bothers me, i have added photos of the joint replacement prosthesis. My second question is: intra oral placement risks infection, not just of the implant, but also the artifical jaw joint, which would be pretty bad. Would a extra oral approach significantly reduce the risk of infection? I saw some studies on hip and knee replacement giving a number of 0.3-1% infection rate which is extremely acceptable, would this number be comparable to a jaw implant placed extra-orally? Some sources ive found have stated that extra vs intra orally placement of chin implant is only 1% vs 2% risk, that barely seems to make a difference in route of placement. My last question is, would the jaw angle implant be delivered through a new scar, or would the same scar be opened up to place the jaw angle implant.
A: I don’t think there is any question that if you had indwelling TMJ joint replacements with the external approach to put them there would be no reason why you would not use the existing external scars for jaw angle implant placement…which would appreciably lower the infection and make the recovery easier by staying out of the mouth. In addition custom jaw angle implants would be needed so they mesh with the lower end of the condylar prosthesis and better manage any asymmetries between the two sides which will inevitably be present.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am contemplating this temporal reductio b surgery. My skull is already wide and in addition those muscles are very prominent on me. My hairline is also thinning on the sides which has been exposing them even more Into my mid 40s. I was also wondering about a jowl lift and how much that will benefit me in the long run if I got one this early in life. My mother’s are very pronounced and mine are getting there but, I’m only 43. I thought I should at least ask if I end up going for the temporal reduction anyway. Do you have any suggestions or recommendations for me? Thanks
A: Thank you for your inquiry and sending your pictures. I believe you are referring to the temporal reduction surgery in which the posterior temporal muscle is removed which appreciably narrows the side of the head. It is actually a very uncommon requested procedure for females because of hair coverage on the side of the head but how the operation is performed and the merits of doing so remain the same.
What you are referring to for the early onset of jowling is a jowl-tuckup type of lower facelift…what I call a Level 1 Facelift. (some call it a ‘mini’ facelift etc) You are at the right age for this type of limited lower facelift in which patients want to get early correction to keep the jawline and neck clean and smooth.
Temporal reduction and any form of lower facelift surgery can be combined if the patient so desires.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What exists for myself is well over 10mms of temporal contour excessand I know removing the posterior temporal muscle completely would make immense changes in my appearance. I’m based in Australia and I’m truly surprised that you’re the only surgeon going around that offers this procedure so I’m considering of traveling over. Have you had patients travel to you from overseas before?
Just a couple of questions, can you by any chance perform more than one procedure in one operation? I’m questioning that because I want a brow bone reduction done as well as a posterior temporal reduction done on myself.
A: In answer to your temporal and brow bone reuction questions:
1) The vast majority or my practice is with patients who did not live where I am located. So geographically distant patients, including patients from Australia, is the norm not the exception.
2) Brow bone reduction can be performed at the same time as temporal reduction. The key question is what technique is needed to do it. But regardless of technique it can be performed during the same surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a dime size dent in my brow/forehead area from forehead reconstruction surgery, I had done 3 years ago. I was wondering how much for bone cement in that area?
A: Thank you for your inquiry. Bone cement is one option for placement into the brow bone defect…but not the only option. That is a difficult area to get bone cement into without wide open access. The concept of injectable bone cements would not apply to a brow bone defect area for a variety of reasons. Thus I would opt for an endoscopic approach where ePTFE (Goretex) sheeting could be more easily and reliably placed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley ,Hi, I’m 25 years old and have had hollow under eyes all my life. I used to think it was just thin skin but I’ve realized I believe it’s a suborbital deficiency after seeing images. I wanted to see if I would be a better candidate for filler, fat transfer or a suborbital implant. My dermatologist said she wouldn’t do filler on me because under eye filler migrates. I also attached a photo of me at 19 showing a particularly bad photo of the hollows.
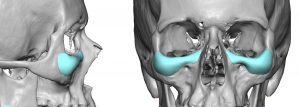 A: Thank you for your inquiry and sending all of your pictures. When you have significant undereye hiollows due to a bony deficiency, which is almost always the cause of significant undereye hollowing, the most significant improvement with the longest duration of effects is going to be a suborbital implant. Or more specifically custom infraorbital implants made from the patient’s 3D CT scan. To optimally correct the bony deficiency it requires an implant design that creates both horizontal and vertical augmentation of the infraorbital rim which no standard implant can do. (see attached)
A: Thank you for your inquiry and sending all of your pictures. When you have significant undereye hiollows due to a bony deficiency, which is almost always the cause of significant undereye hollowing, the most significant improvement with the longest duration of effects is going to be a suborbital implant. Or more specifically custom infraorbital implants made from the patient’s 3D CT scan. To optimally correct the bony deficiency it requires an implant design that creates both horizontal and vertical augmentation of the infraorbital rim which no standard implant can do. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, how long does it take for hair to start growing through a trichophytic incision, and once it does, how short can you wear your hair?
I am a male and about a year ago I had forehead contouring surgery through a bicornal incision and they utilized a trichophytic incision. They hair never seemed to grow through and I had two big visible scars down the sides of my head. I just had a scar revision a month ago with another trichophytic closure and there still are visible lines down the sides of my head and there’s only very sparse hairs through the scar.
A: You will find getting a good scar result in the temporal area is very challenging and it is almost better to hair transplant it if this scar revision ‘fails’. Hair should be growing through the scar line within one to two months after surgery…if it is going to do so at all.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering are infraorbital-malar silicone implants inserted through a transconjunctival incision or intraoral? Thanks.
A: Those are two incisional options for custom infraorbital-malar implant placements both of which are associated with a higher risk of infection (intraoral), implant malposition (intraoral and transconjunctival) and infraorbital nerve injury. (intraoral) Whether those incisions are even options worth considering depends on the extent of the infraorbital part of the implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question for about lateral orbital rim rimmorbital augmentation using bone cement. Does it work and could you do that please.
A: Bone cement is very hard to place in a complete and smooth manner at the lateral orbital rim through a small eyelid incision. It is not a question as to whether it can be done but whether that is a good technique to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, With regards to skull augmentation, instead of placing implants under the skin, would it be possible to extend the bone and place implants or some kind of bony material in place of the gap in between the bone when it gets split open? For instance, you can extend the forehead by making a horizontal incision on the frontal bone and extending the top portion above the cut, and then fill the empty space with something. If hair gets uneven, there can be hair transplants done. What are your thoughts?
A: That is not a viable skull augmentation concept. If you separate the outer layer of the bone and place a synthetic barrier between it and the underlying bone the detached bone will die/atrophy as it has no blood supply.
This concept also does not account for smooth contours around all edges of an augmented skull areas which is one of the primary determinants of a favorable aesthetic outcome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Rib Removal and Clavicle Reduction surgeries. I had a few questions :
– what is the expected reduction in waist size for rib removal (width and circumference)?
– does you have experience with comparing outcomes between the two procedures?
A: In answer to your questions:
1) Rib removal patients report an average of 1 to 3 inches in circumferential waistline reduction. (by the patient’s own measurements) I focus more on the improvement in shape or how it looks.
2) Clavicle reduction is very different and is a completely predictable operation in terms of outcome because the amount of clavicle bone removed correlates 1:1 with the visible reduction in shoulder width. Thus if 2.5cms of bone is removed per side than the shoulder width reduction is 1 inch per side.
The difference is that the clavicle bone is linear in orientation and the reduction is completely dependent on the bone length removed. Conversely, the lower ribs are oblique in orientation and the length of bone removed does not correlate to the horizontal waistline reduction directly. In addition waistline shape/circumference is controlled by more than the just bone with a substantial contribution of soft tissues as well.
Dr. Barry Eppley’
Indianapolis, Indiana
Q: Dr. Eppley, I have had two chin implant surgeries intraorally and considering a revision to a custom chin implant. If I were to proceed with a custom implant, is there a way to improve the tightness in the labiomental crease as part of the revision surgery? I have heard fat grafting to this area can be helpful. If that’s true, what type of fat graft would work best? I am a thin woman so I don’t know how much fat would be needed (I don’t have much). Would it be worth the risk of another intra-oral surgery to try and get this improvement? Does this add a lot of cost and time to the procedure? Thank you for your advice.
A: Injection fat grafting to the labiomental crease can be performed at the same time as a chin implant replacement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, hello, I am wanting to have a sliding genioplasty done. I had a consultation with an oral surgeon and was told that one of the risks are that two small grooves on either side of my chin my occur as a result. She recommends advancing 9mm. But i wanted to ask you in terms of your technique is there something that could be done to avoid these? Does the amount of advancement play a role in the dents? i appreciate your time, i am just looking to make the right decision.
Thank you.
A: Inferior border notching is an inevitable sequalae of most sliding genioplasties. The larger the movement the more likely it will occur. Suffice it to say at 9mms you can assume it will occur. There are ways to lessen it such as a low angled osteotomy cut or concurrently filling in the notch with various types of grafts/materials.
The question is not whether it will occur but whether it will turn out to be aesthetically bothersome and whether any of the intraoperative strategies can sufficiently reduce/eliminate the notching.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young Asian female. My main concern is I have prominent chin and my mid face is flat , I had braces when I was a teenager, now my bite is correct , but I still have a crescent moon side profile . I ‘d like to got consultation to get a better opinion on is it possible to achieve result to the photo with the help of paranasal implant and jaw reduction surgery . I attached the before and after pictures also my X ray , I am wondering if the after results are possible?
A: Thank you for your inquiry and sending your front view imaged picture. Certainly a single (paired ePTFE paranasal implants alone) or double stacked (paranasals + premaxillary overlay) implant can nicely augment your central midface as your imaging has shown. For the jaw reduction there are numerous techniques to do it and which one is best for imaged result remains to be determined but at the least an intraoral t-shaped chin reshaping procedure is needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q; Dr. Eppley, Im interested in fat transfer to brow and temple and/or non invasive brow lift (not botox) and fat graft to the hands. I had a mini lower facelift several years ago and just had an upper eyelid lift this year. My eyelids are still heavier than I’d like because my brow needs to be lifted. I’m not a candidate for endo brow lift because I have a high hairline and family history of hair loss.
A:I am not aware of what a ‘non-invasive’ browllift may be as they are all surgical. Excluding an endoscopic browlift every other browlift works by the excision of tissue somewhere to achieve its effect. For a high hairline patient the only options are a pretrichal (frontal hairline) or a direct browlift approach. While fat grafting will add volume to the brows it is not going to create a true browlift effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can you do the skull reshaping procedure? I want my skull reduced because I have extra grown two horn-like bones on top corner of both sides of the head. This made my head shape really awkward like an Alien shape, has made me insecure throughout life, made me lost confidence in many things throughout growing school days, teen to adult days etc. Now am seriously looking to get this sorted and I have seen many places from USA and abroad where skull reshaping can be done to some degree.
I would appreciate a response please. Thanks
A:These are skull procedures that I do regularly. (www.skullreshaping.com) Can you please send pictures of these horn-like protrusions for my assessment.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Would it be possible to decrease the distance between the eyebrows by removing a portion of skin between the eyebrows right above the nose bridge in a sort of sideways (american) football shape and then stitching the wound closed, pulling the skin and therefore eyebrows a few mm closer together?
A: That would be one way to do it although hair transplants or micro pigmentation would avoid the vertical glabellar scar.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a facial feminization surgery scheduled in the fall. How long would I need to wait after this surgery to be safe to be in the ‘facing down’ position for the rib removal surgery?
A: I would wait a minimum of 3 to 4 months after facial feminization surgery so most of the healing is complete before having one’s face be positioned into a soft cradle for rib removal surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if the hydroxyapatite paste you use in the chin surgeries turns into bone later? Or does it just become hard but not into bone?
A:I don’t use hydroxyapatite paste in chin surgeries since it is a ceramic and never turns into bone. What I use is allogeneic corticocancellous bone chips and blocks which can turn into the patient’s own bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is bilateral temporal reduction risky? Does it have any history of affecting you. How long does the surgery last?
A:Temporal reduction is a perfectly safe surgery that has no adverse effects. Because it is a reductive procedure its effects are permanent.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley I had breast augmentation last year but my right breast is doesn’t look like left one, my right nipple 1 cm lower then left one, I just wondered that can we do crescent breast lifting for my right breast lower nipple. Because I don’t want big scars.
A :It is important to remember that all breast implants do is take one’s natural breasts and make them bigger. Thus asymmetries like yours (horizontal nipple level differences) after breast augmentation are usually what the breasts looked like before the surgery…but often not noticed because the breasts were smaller and the difference between them less as a result. The corrective approach, as you have noted, is a superior areolar crescent lift.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a very weak chin (I think) and was curious what you would recommend as the best course of action?
A:Thank you for your inquiry and sending your pictures. Your chin is weak but not in the traditional horizontal manner. Rather the chin and entire jawline is vertically deficient. This is also associated with a short neck and low hyoid position. There are two approaches to take with your lower face which depends on whether you want just the chin changed or the entire jawline. If it is just the chin then a vertical lengthening bony genioplasty would be the best procedure. If you desire the entire jawline treated then a custom jawline implant would be the procedure. What would separate these two procedures, besides the extent of the jawline treated, is how much vertical lengthening can be achieved at the chin. (the bony genioplasty can do more) These differences are best seen in the frontal view imaging.
Either procedure needs to be combined with neck management (submentoplasty) for the best result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in hip pelvic implants but not the kind that are simply stuffed into a pocket, I’ve been to numerous doctors and the only type of procedure they do are standard hip implants stuffed in a pocket. I have contacted a hospital in Seoul that is known for pelvic plasty but noticed one of your replies on Real Self in response to a similar inquiry. I am very lean and narrow hips and are looking to round out my figure. I am also a trans woman which only adds to my hip deficiencies. I have attached photos for your review. Look forward to hearing back from you! Thanks so much
 A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. This is a procedure known as Pelvic Plasty. Until recently only South Korea offered such pelvic widening implants made of titanium…which is the ideal material for augmenting the bony iliac crest given their side position on the bone and the external forces to which they are exposed. In April 2024 the FDA approved the titanium iliac crest plates used in Pelvic Plasty for clinical use here in the U.S.
A: Thank you for your inquiry and sending your picture. The type of hip augmentation to which you refer is that of iliac crest implants which provides a bony augmentation to the upper hip region rather than a lower soft tissue augmentation over the greater trochanteric region of the hips. This is a procedure known as Pelvic Plasty. Until recently only South Korea offered such pelvic widening implants made of titanium…which is the ideal material for augmenting the bony iliac crest given their side position on the bone and the external forces to which they are exposed. In April 2024 the FDA approved the titanium iliac crest plates used in Pelvic Plasty for clinical use here in the U.S.

 I recently (August 2024) started perf0rming the Pelvic Plasty procedure which has become a composite approach combining titanium iliac crest plates with sub iliac silicone implants that attach (hook into) the under side of the plate.
I recently (August 2024) started perf0rming the Pelvic Plasty procedure which has become a composite approach combining titanium iliac crest plates with sub iliac silicone implants that attach (hook into) the under side of the plate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have plagiocephaly (flat head syndrome). because of this, my head from front view looks wide and makes it impossible for me to wear caps. I want a little parietal bone reduction on the sides above my ears only… No matter how little it can be trimmed, i will appreciate that. Please i need your help urgently as this is bothering me a lot.
A:Thank you for your inquiry. Parietal bone reductions are done through a small vertical incision over them. The maximum amount of bone thickness is always removed which is in the 5 to 6mm thickness range.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a surgery, dermal graft and testicle implants but it didn’t work. I lost part of the dermal graft because one got infected. Regarding implants… I don’t like them because they’re too small and I can see 4 testicles as I have too much skin. So I would like “the bigger the implants” you can put (7.5 or even 8cm if it was possible) Because I have a lot skin and I would like that new implants to hide my real testicles. In fact, I don’t mind if my scrotum is tight or if my testicles go to up due to new balls. I like that. Don’t worry about that.
A: Thank you for sending your pictures. I would agree that 7.5cms size implant replacements would likely push your natural testicles out of the way and make them less visible. The current implants you have are too small and have done what I would think would have happened…show all 4 of them.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley,After a few months after my buccal lipectomy I am thinking I want to reinsert fat back into my buccal area. Just not satisfied with the look, my face just looks too skinny. I probably just should’ve went with the buccinator myectomy and perioral mound liposuction initially, can’t change the past and can only move forward. My question is how to reinsert fat back into the Buccal area and how many ccs of fat is needed to fill the area back up properly? Thanks
A: There are two ways to restore buccal fad pad volume which is in the 2cc to 3cc range, fat injections or the insertion of en bloc (solid) fat graft back into the buccal fat pad space. Each method has its advantages and disadvantages. Usually the latter is more effective as it puts the volume directly back into where it was initially removed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is sliding genioplasty an option to improve jawline/chin structure? I don’t want to have more major jaw surgery, since I don’t have the ability to take that much downtime off work. Also, I have no bite problems and no sleep issues. If sliding genioplasty is an option, I would be interested to see how much it could potentially help.
Thank you in advance!
A: Thank you for your inquiry and sending your pictures, You are correct in that short of a major lower jaw advancement a sliding genioplasty would be the correct procedure not a chin implant. The chin bone needs to move as far forward as possible, maybe even being a jumping type of genioplasty to maximize the forward movement and avoiding adding any vertical length to the chin. This would have the same aesthetic effect as moving the lower jaw forward with the exception of the position of the lower lip and the depth of the labiomental fold. (which can only be improved by the lower jaw advancement since these are teeth-based positioned structures) I would also do liposuction of the neck to enhance the effect of the chin advancement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I might be interested in the bicep implant. Maybe you can give me some more information on cost and if there are any scars after the surgery.
A: Thank you for your inquiry. There are two approaches to the placement of a bicep implant, on top of the muscle under the fascia (subfascial) or under the muscle on the bone. (submuscular) There are advantages and disadvantages with either implant location. There are also different incision locations between them as the subfascial technique puts the scar high up in the axilla and the submuscular technique puts a small incision in the inner arm area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in having Forehead Augmentation Surgery. I am a transgender woman and I have had my brow bone shaved down. While it improve my appearance, it still did not give me the forehead I am looking for. I want to achieve a more rounded/flat, feminine forehead, right now mine has a slope that is not appealing in a female.
I have read that the most common approaches are bone cement and custom-made implants. I am interested in learning how much this type of surgery would cost (both with bone cement and implants), and how long would I need to stay in the area.
I am attaching four images, one showing my current profile, another one showing what I would like to achieve, and two more images of a CT Scan that I recently had done showing the anterior and lateral side of my head.
Thank you very much for your attention to my inquiry.
A: Thank you for your inquiry and sending your picture. You are correct in that ‘old style’ bone cements and contemporary custom implants are the two most commonly used options for forehead augmentation. There is also a newer standard ePTFE preformed forehead implant. Each has their advantages and disadvantages which ultimately comes down to what incisional access is needed to place them, how far back along the upper forehead and to the sides of the forehead does the augmentation need to cover, how precisely can each method achieve the aesthetic forehead goals in a smooth and even fashion and their costs to perform them.
Because of your prior surgery you undoubtably have a long frontal hairline or more posterior scalp scar for access so the incisional differences between the forehead augmentation methods is irrelevant. If you throw out costs the custom forehead implant is always the best choice because you control every dimension of the implant prior to its placement so achieving the final goal in a smooth manner with no edging is the most assured. Bone cements are also a good option for you because you need to be able to turn down the forehead flap so an open visual field exists to apply, shape and let the cement cure. This requires the long incision which again I assume you have. There are two different types of bone cements, PMMA (plastic) and HA. (hydroxyapatite) HA is the best bone cement to use because it is composed of inorganic calcium phosphate crystals which is the most similar to bone…but it has a significant cost factor to it. PMMA is the most economic bone cement option. Off-the-shelf PTFE (Goretex) forehead implants are used primarily for the Asian female who wants a rounder forehead and limited incisional access to do so. But they are more a central forehead augmentation method.
If you look carefully at your own side view imaging prediction notice that the frontal hairline remains the same indicating that the augmentation shown is more of a central augmentation effect that only needs to feather out as it approaches the hairline. (and probably the bony temporal lines as well to the sides) Given your more central forehead augmentation goals (which are probably in the 5 to 7mm increase at most) and keeping an eye on costs, bone cements vs a preformed ePTFE forehead implant are good choices for you.
As for logistics you would fly in the afternoon/evening before surgery, have surgery the next day and then fly home the following day.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am very unhappy with how long/big my head is. I am wanting to inquire about a skull reduction procedure, and specifically reducing the size of the back of my head; seeing if what I would like done is even an option.
Thank you for your time.
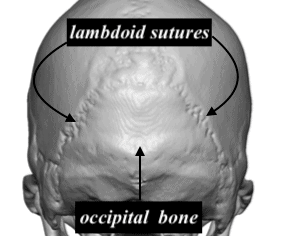 A: Thank you for your inquiry and sending your picture. You have a classic occipital bone protrusion whose border is the lambdoid sutures. This is where the occipital bone grows outward out of proportion to the adjacent parietal and temporal bones, hence the protrusion. The occipital bone can be reduced and brought back into alignment with the surrounding skull as the per attached illustration.
A: Thank you for your inquiry and sending your picture. You have a classic occipital bone protrusion whose border is the lambdoid sutures. This is where the occipital bone grows outward out of proportion to the adjacent parietal and temporal bones, hence the protrusion. The occipital bone can be reduced and brought back into alignment with the surrounding skull as the per attached illustration.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am writing to you as an expert in male facelifts that are bald. I am interested in knowing if I am a good candidate for the surgery. (pictures attached)


 A: Thank you for sending your pictures. I am not certain what qualifiers one as a ‘bald male facelift expert’ but I have certainly done a few such patients. The basic maneuvers of a facelift remain the same but with the caveats of some alterations of incisional placement around the ears. It is important that the anterior ear incision not go above the helical root and descends to the earlobe in a retrotragal fashion and that the posterior ear incision and backcut not go beyond the shadow of the outer helical rim. The submental incision for the central neck work remains the same as in any other patient. The key to any male facelift, and the bald/shaved head patient in particular, is to have little to no evidence around the ears that the surgery was done. Limiting the incisions around the ear does compromise how ‘aggressive’ the facelift result can be but I think most men will settle for visible improvement of their neck/jawline with no minimal scarring vs a perfectly tight jawline and 90 degree neck angle with visible scarring.
A: Thank you for sending your pictures. I am not certain what qualifiers one as a ‘bald male facelift expert’ but I have certainly done a few such patients. The basic maneuvers of a facelift remain the same but with the caveats of some alterations of incisional placement around the ears. It is important that the anterior ear incision not go above the helical root and descends to the earlobe in a retrotragal fashion and that the posterior ear incision and backcut not go beyond the shadow of the outer helical rim. The submental incision for the central neck work remains the same as in any other patient. The key to any male facelift, and the bald/shaved head patient in particular, is to have little to no evidence around the ears that the surgery was done. Limiting the incisions around the ear does compromise how ‘aggressive’ the facelift result can be but I think most men will settle for visible improvement of their neck/jawline with no minimal scarring vs a perfectly tight jawline and 90 degree neck angle with visible scarring.
While longer scars that trail away from the ears do allow for more skin removal/tightening and better results, there is no forgiveness/improvement when such scars are done. This is an example of a patient that came to me with such facelift scars. No scar revision will ever make them go away. This is what one wants to avoid.
Dr. Barry Eppley
Indianaoplis, indiana