Your Questions
Your Questions
Q: Dr. Eppley, I have a chin that is a little but long when I smile. Also I feel my chin is a bit short. I would also like liposuction under the chin at the same time. What would be the approach for optimal correction?
A: Thank you for your inquiry and sending your picture. In the chin that has a dynamic chin pad ptosis in which it is also a bit horizontally short, a chin implant placed through a submental incision (not intraoral) is the corrective approach. Submental/neck liposuction can be performed at the same time through the same access incision as the chin implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can shoulder narrowing surgery and hip implants be done at the same time? This has some obvious advantages in terms of efficiency but what about the recovery?
A: The question is not whether one can have both shoulder narrowing and hip implants done at the same time, as that can be done technically, but whether it makes the recovery very difficult in he short term. (which it would)
From that perspective it makes sense to do the hip implants first (as it requires laying on your side for each side and requires a drain which needs to stay in for awhile) and then the shoulder reduction. Or do them separately months apart when one is fully recovered from the first procedure.
I hate to separate them as described due to the logistical impact on the patient but i also don’t want to put a patient into an adverse and very difficult recovery. Each procedure affects mobility from their respective upper and lower torso involvements. It is one thing to affect one torso range of motion/movement but it can be quite another when the entire torsi is affected. (high and low)
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley, I am a young man who is due to undergo bimaxillary advancement for health reasons. The planned procedure involves a Le Fort 1 osteotomy. I have researched this topic in depth, so I am aware the different Le Fort osteotomies and their aesthetic implications. I have learned that I not only have a recessive lower maxilla, but my entire nasal region (both upper and lower) is recessive. I understand that this is the area moved foward with a Le Fort 2 osteotomy. I now have to make a choice between going forward with the Le Fort 1 osteotomy, or scrapping my plans and finding a surgeon who would perform the full Le Fort 2 osteotomy. The key aspect that will inform my decision is whether it is possible to (almost) achieve the results of a Le Fort 2 osteotomy with a combination of a Le Fort 1 osteotomy and a customized implant (or more than one of them). I envisage the customized implant to move forward the entire circumference of the piriform aperture in addition to the nasal bone and the frontal process of the maxilla. If this is possible, I would come to you for this implant after undergoing bimax. What do you think about this?
A: It is important to remember that facial bone surgery is not always as it appears in a diagram. LeFort II and III osteotomies look great on a diagram but executing them and accepting the tradeoffs and their more limited aesthetic effects is a different matter. The more assured result is a LeFort I, which is a very predictable operation, followed by addressing the remaining superior aesthetic midface needs secondarily with custom implants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an orchiectomy nearly twenty years ago due to an undescended right testicle. I have an implant which I have never found satisfactory. It is too small and has been stitched in place, so it does not hang or appear correct. I’m interested in your much larger implant. Can you please provide more information? I am desperate to have a better implant that looks more satisfactory.
A: Thank you for your inquiry and sending your pictures. Undoubtably you have a small saline testicle implant which it is sutured in placed using a permanent suture through a tab on the implant. (why Urologists do that I do not know) Because it is saline-filled is why it is very firm.
To create a soft more mobile implant it needs to be replaced with an ultrasoft solid silicone implant probably of a size of 5.5cms which would be a much closer match to the remaining testicle, if not a bit bigger. The suture needs to be removed and the residual capsule released with the new implant placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in fat injection breast augmentation. Attached are a few photos that I took this morning. As for the breasts I do not want large breasts, I just want to fill out the skin that I have. You can see in my side profile that the top half is pretty flat and empty. i like the look and feel of natural breasts which is why I am more interested in fat transfer but I am not completely opposed to a small implant if we can keep them natural looking. I do not like the look of my indentions in my hips. I have had them for as long as I can remember, no matter how small I was. I do like the curvature of my body in my waist so I would like to have liposuction of my tummy and use the fat to fill in my hips so that I have a smooth curve. In the last photo you can see that I have a small overhang of belly skin, I do not want a tummy tuck because I do not want to be left with a large scar. I have heard of SkinTite being used with liposuction to help reduce this and wanted to know if you offer that or have any other suggestions.
A: Thank you for sending your pictures to which I can say the following:
1) While you do have some fat to harvest any amount of fat injected into your breasts is not going to round them out or provide the upper pole fullness you lack. Fat works best in breasts that have a good skin sleeve/tightness. It doesn’t have the stiffness or push, no matter what the volume injected is, to have an expansive effect in the breast with loose skin. Only an implant can provide the push needed to have that effect.
2) Thus fat harvested would be better used for the hips even though that is a notoriously poor area for injected fat survival. But enough volume injected can overcome much of that anatomic unfavorability.
2) While you can have liposuction, which will have some reductive/flattening effect on your stomach, there is no benefit to the use of SkinTite afterwards as the ability to tighten skin that has stretch marks is negligible. You have to rely on whatever natural skin elasticity remains in which yours is limited.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I know you claim the buccal myectomy produces just modest results but for a highly motivated patient that is willing to accept risks, would you be able to remove more and tighten more muscle for a more dramatic result?
What kind of risks are there if you try to tighten more?
A: I suspect the main risk with an ‘aggressive’ buccinator myectomy would be excessive tightness of the cheeks. (scar contracture)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, So I have a very small head. So small that I’m convinced I have the smallest head on earth for a healthy adult male. I know for sure it’s smaller than 54cm. I have a few questions about this procedure but rest assured I will be making an appointment in the future.
How much does the surgery cost? That way I know how much to save
What can I do in the meantime to maximize the enlargement potential? Collagen supplements?
Will there be scars? If so where? Will the cuts be anywhere hair is located?
I’m worried the head enlargement will throw off the rest of my features. If so will there be an option to enhance those as well?
A: In answer to your head enlargement questions:
1) The cost of head enlargement surgery depends on how it is done. (one vs two stage)
2) Head enlargement surgeries are maximized by doing a two stage approach which employs a first stage scalp expansion which permits a larger implant to be placed.
3) The scalp incision is usually placed near the crown of the scalp.
4) Most head enlargement surgeries are probably not going to be big enough to make the face look too small.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi! I love your work and I am very interested in your shoulder narrowing surgery! Have you done any cis-gendered women? Also, do they end up looking hunched over? Thank you !!!
A: About 25% of shoulder narrowing patients are cis-females so they do request the procedure just not as much as the transgender patients.
Patients do not develop a hunched shoulder appearance afterwards. That is only a posture you see in the early postoperative period because it is the most comfortable position for the shoulders. It also results from keeping the elbows close to one sides in the first few weeks after surgery to protect the healing clavicle osteotomy sites.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The testicle implant I have was placed nearly twenty years ago. My actual testicle size is about 3.5 – 4 Cm approx….I used a simple ruler to measure them. I would like to get a large implant for both sides to improve size and also a softer and natural to the touch.
You suggested new size implants of 5.5 Cm for both sides. Are these medium or large implants?. I’m a little concerned that a 5.5 Cm wraparound might strangle my actual testicle. Is it possible? Is it better unrestricted or restricted? No dancing around in the wraparound. I’m looking for the perfect fit physically and visually and since I have a small frame, nothing ridiculous, too big .. 🙂
Thank you so much again!
A: In answer to your testicular implant questions:
1) Most likely your natural testicle size is about 4 cm+. I assume the testicle implant is smaller, probably more in the 3 cms size range.
2) The largest standard off the shelf testicle implant is 5 cms. Most men who get testicle implants would still consider that ‘small’. Thus either 5.5 seems reasonable for both sides as that is an upgrade but not by an unreasonable amount.
3) Wrap around testicle implants do not strangle or compress the existing testicle or the attached cord. In fact the risk with them is the opposite of your concern…having the testicle slipping out of the wrap around implant. That is why they are sutured into the implant to prevent that potential postoperative issue.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a male and I was wondering if u could fix my asymmetrical face and one of my eye brows go up higher than the other side and on one side of my lip is bigger than the other side and the other side of my face is sagging than the other.
A: Thank you for your inquiry and sending your picture. What you have is a right side of the face asymmetry caused by a developmental shortness on that side compared to the left side. That is most manifest mainly by the right vertical orbital dystopia (right eye lower than the left eye) which is the cause of the lower right eyebrow. Like all facial asymmetry corrections it comes down to determining what is most important to improve vs the tradeoffs (scars) in doing so. What I tell all my facial asymmetry patients is to make a liost of thge priorities so I can go through it with them and discuss what can be done and the potential tradeoffs in doing so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a male and I was wondering if you could fix my asymmetrical face and one of my eyebrows go up higher than the other side and on one side of my lip is bigger than the other side and the other side of my face is sagging than the other.
A: Thank you for your inquiry and sending your picture. What you have is a right side of the face asymmetry caused by a developmental shortness on that side compared to the left side. That is most manifest by the right vertical orbital dystopia (right eye lower than the left eye) which is the cause of the lower right eyebrow. Like all facial asymmetry corrections it comes down to determining what is most important to improve vs the tradeoffs (scars) in doing so. What I tell all my facial asymmetry patients is to make a list of the feature priorities so I can go through it with them and discuss what can be done and the potential tradeoffs in doing so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want to ask Dr Eppley 3 quick questions regarding brow bone reduction.
– what is the average bone thickness over the frontal sinus?
– how much bone can we shave over the frontal sinus? (in mm)
– and what is the minimal bone thickness we can let over the frontal sinus?
(without risks of tissue dying)
A:In answer to your brow bone reduction questions:
1) The average of the frontal sinus table in men is 3mms.
2) Since 1mm needs to be left, 2mms can be reduced by burring.
3) As stated in #2, 1mm.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, If the effect of temporal muscle injection is relatively small, can the anterior temporal bone and the posterior temporal bone be erased about 1cm by bone grinding? At the same time, I have another question, that is, the zygomatic arch, temple and forehead in my CT are relatively wide, can I remove about 1cm of bone on both sides by bone grinding? Thank you very much!!
A :How do yo know that the effect of temporal muscle reduction is small/inadequate? The temporal bone is fairly thin so a 1 cm bone reduction is not possible.
As for the forehead/temporal/zygomatic arch, a 1 cm per side reduction can not be done as the bone is not that thick. More realistically it is 5 to 6mms per side for a 1.0cm collective cheek width reductions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, In regards to the Pelvic Plasty procedure (iliac crest implants) where is the incision made to place them and what type of scar does it leave?
 A: The incision for iliac crest implants is made at the posterior iliac crest region and is about 3 cms in length. This requires the surgery to be done in the prone position. (face down) The incision is made in the panty line so it is in a good location for being hidden in underwear. It is closed for fine sutures using a subcuticular suture technique in which all sutures are buried under the skin. As a result they don’t need to be removed and also leaves no suture track marks. It usually heals as a fine line scar and rarely requires the need for scar revision.
A: The incision for iliac crest implants is made at the posterior iliac crest region and is about 3 cms in length. This requires the surgery to be done in the prone position. (face down) The incision is made in the panty line so it is in a good location for being hidden in underwear. It is closed for fine sutures using a subcuticular suture technique in which all sutures are buried under the skin. As a result they don’t need to be removed and also leaves no suture track marks. It usually heals as a fine line scar and rarely requires the need for scar revision.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I was wondering if it would be beneficial to do the Scrotox injections to keep things relaxed while healing from getting large testicle implants? Worried about the incisions being pulled due to the natural swelling that will occur after the surgery. Maybe not a issue but curious…
A:Incisional dehsicence has never been a problem in large testicle implants in my experience so I think the expense of Botox injections may not be a good expediture. It certainly does not hurt but am not sure if the benefits are worthwhile.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I shave one eye lower than the other one and it has been so since birth. After researching on the internet I believe I have Vertical Orbital Dystopia. What can be done to make my eyes more symmetrical in appearance?
A: Thank you for your inquiry and sending your picture. To learn in detail what can be done for moderate VOD I would refer you to one of my websites, www.exploreplasticsurgery.com where you can place in the search box the term Vertical Orbital Dystopia and read the various articles about its surgical treatment. The first step in the process begins with obtaining a 3D CT scan of your face so the measured differences between the two orbital boxes can be determined.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I really appreciate your medical service. Thank you for posting superior medical job at this site. I`m living at Asia and preparing for MTF surgery. I have two questions about body contouring surgery.
First, how long should I stay for healing process? (Essential hospitalization term) Second, Which surgeries can be done at once? For example, subcostal rib removal and shoulder reduction go on first and later rib removal. Or all at once. Also if none of them can`t be done together, please tell me.
Once again, I feel truly thankful that your hospital provides such a beautiful surgery.
Thank you for all.
A: Thank you for your inquiry. In answer to your questions:
1) Shoulder reduction and rib removal can be performed together in the exceptionally well qualified patient but we will assume for now that they would be done separately.
2) The subcostal rib removal procedure can be combined with either shoulder reduction or rib removal. Whether that is a good procedure for your remains to be determined.
3) When to return home from either procedure partially depends on whether you are traveling along or with someone. For now I will assume the former. Thus for shoulder reduction one could return home 10 days after surgery. For rib removal it would be quicker in the 4 to 5 day time period.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How many custom implants can be placed in one session? Is it possible for chin, jawline, zygomatic arch and temporal implants in one session?
A: Placing multiple custom facial implants during the same surgery is common in my experience. I have seen as many as ten custom skull and facial implants placed in a single surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been looking for plastic surgery for supraorbital augmentation because my eyes are like Asian eyes and i like caucasians eyes. The Caucasian supraorbital bone covers eyes and it makes the deep and shadowed which I find attractive. It sounds like that I am trying to change my race. But if i can do the surgery i want to get the surgery So my question is “is it possible” ? Thank you for reading my text.
A: What you are referring to is brow bone augmentation, sometimes referred to as supraorbital rim augmentation, which I do with a custom brow bone implant. While it is more commonly done in males there is no reason it can not be done in females as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, For a long time I have had some major insecurities with forehead. I liked my look but not side profile.I went to a FFS doctor to do a forehead reduction since I felt it was so masculine and people have always said I look different from my side profile and this was a huge problem for me. I could not even wear sunglasses because my forehead stuck out too much. I told the doctor to not remove to much bone, nothing from my forehead but only the bone you take out and put in. I said to him to not shave my brow bones to much since I like my look around my eyes and to NOT give me the «surprised look»
My brow bione is almost completely shaved and not existing. I am so so so sad, and this has ruined my whole facial expression. I have been deeply depressed since the surgery.. I found you and you brow bone implant, and I think now you are my only hope to get back my look and protection around my eyes. Is it possible to fix this?
 A: Thank you for your inquiry and sending yiour pictures.You unfortunately represent an overcorrection brow bone reduction result. Fortunately it can be improved/partially reversed by a custom brow bone implant. To avoid going completely back to where you started you probably only need a 3 to 4mm thick implant at most. Attached is an example of such an implant footprint although your implant thicknesses would be different. You already have the access incision to place ot of which scar revision could be done on it at the same time
A: Thank you for your inquiry and sending yiour pictures.You unfortunately represent an overcorrection brow bone reduction result. Fortunately it can be improved/partially reversed by a custom brow bone implant. To avoid going completely back to where you started you probably only need a 3 to 4mm thick implant at most. Attached is an example of such an implant footprint although your implant thicknesses would be different. You already have the access incision to place ot of which scar revision could be done on it at the same time
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I am just inquiring if you are able to correct SCAPHOCEPHALY, which is when the head shape is slightly narrow and abnormally long?
If so, are you able to help children and adults?
Thank you
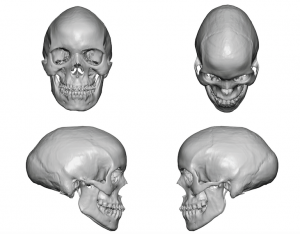
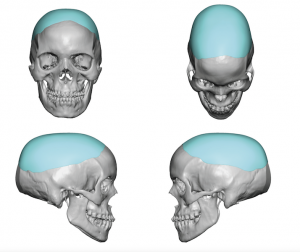 A:I do have an approach to treat adult scaphycephaly as seen in the attachments which consists of some anteroposterior bone reduction and widening skull augmentation by a custom skull implant.
A:I do have an approach to treat adult scaphycephaly as seen in the attachments which consists of some anteroposterior bone reduction and widening skull augmentation by a custom skull implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a tummy tuck 7 weeks ago and I am concerned the results are below my expectations. I found your details through a google search and am wondering if you can give me your opinion please
I had liposuction, muscle tightening/stitches and skin removed from the upper and lower abdomin.
I would have expected to have a pretty tight and flat abdomen by now but I still have cellutite and soft skin that I can grab handfuls of. My weight and measurements have not reduced and I am quite underwhelmed by the results.
Are my expectations too high? I was told 6 pack definition was not impossible and I am very far away from that result. Will it get better as time goes on or is this as good as it gets?
I have an appointment with my surgeon in 1 week and will express my concerns.
This is the second time I have been through the surgery, as the first time was a complete disaster and the surgeon was happy to redo the work.
I have attached some photos to help explain.
Thank you for your time.
A:Thank you for sending your pictures to which I can add the following secondary comments:
1) You had an inverted T type tummy tuck which was appropriate if the goal was to keep the horizontal part of the scar very low. This type of tummy tuck does not remove as much skin as other more extended types of tummy tucks but less skin removal is the price to be paid for the scar location. A supraumbilical type full tummy tuck would have produced a more significant result with much greater skin removal but at the price of a much higher and longer horizontal scar. The aesthetic danger is this approach in you is that you may have been a lot flatter and tighter but may have hated the scar…in which there is not going back. (aka poor tradeoff)
2) I think your expectations (after this secondary surgery) may have been too high. A 6 pack ab result was never a remotely realistic expectation or anything even close to that outcome.
3) I suspect the fundamental issue here is one of miscommunication or lack of adequate preoperatve education/understanding between patient and surgeon. You are what I would call a ‘tweener’ meaning a traditional full tummy tuck may have produced a better ooutcome but with an unfavorable scar location vs a more limited type of tummy tuck which has a better scar but less of an aesthetic improvement. I am not sure you clearly understood your situation before surgery. In patients like you I go to great lengths in making sure they understand their choice and the involved tradeoffs before the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, I am in love with the results that can be achieved with forehead reshaping/temporal line reductio. I want to do the same for myself. Only problem is I have had hair transplant where they take strip of skin from back of head. So to do the temporal line reduction, I don’t think I’ll be able to do hairline incision like the guy did from the Web page as doing so will drastically reduce blood flow to head. Are you able to do a thin 1-2 cm incision at near ears and then use endoscope to do burring? Or I can do the thin 1-2cm incision right in top of the anterior temporal line. I don’t mind the scar.
Q: Dr. Eppley, I am in love with the results that can be achieved with forehead reshaping/temporal line reductio. I want to do the same for myself. Only problem is I have had hair transplant where they take strip of skin from back of head. So to do the temporal line reduction, I don’t think I’ll be able to do hairline incision like the guy did from the Web page as doing so will drastically reduce blood flow to head. Are you able to do a thin 1-2 cm incision at near ears and then use endoscope to do burring? Or I can do the thin 1-2cm incision right in top of the anterior temporal line. I don’t mind the scar.
A: In answer to your questions about temporal line reduction:
1) The frontal hairline incision has nothing to do with decreasing the blood flow to the head, it is all about the scar.
2) You can not do burring using an endoscopic technique.
3) A more limited incision at the top of the temporal line can be used probably in the 3cm length range.
Dr. Barry Eppley
Indianapolis, Indiana
If I Get Cheekbone Reduction Surgery And Develop A Soft Tissue Sag What Is The Best Way To Treat It?
Q: Dr. Eppley, I am planning to get cheekbone reduction surgery. I have done lots of research and understood and accepted the certain risk of skin sagging. My surgeon recommended me lifting the muscle while doing the cheekbone reduction surgery to precent from sagging. Can this help the sagging? Even if i sag would smas facelift help? Because you mentioned that it is hard to fix skin sagging from surgery with facelift. Thank you.
A:I do not know what ‘lifting the muscle’ means or how that would be done at the time of cheekbone reduction surgery. Once the muscles are lifted off the cheekbones to do the surgery there is no method to put them back.
The definitive treatment for significant cheek sagging is a SMAS based facelift or some form of a lower eyelid or temporal cheeklift.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I have some questions about vertical orbital dystopia (VOD) surgery which I would appreciate if you could answer for me.
1. For VOD surgeries like mine, what risks/complications should I be aware of?
2. Out of all the VOD surgeries you’ve performed, have you seen any cases of severe or irreparable complications (e.g., loss of eyesight, severe nerve damage, etc.)?
3. I got a second opinion from another surgeon, who recommended against an implant, saying it involves too much risk. He recommended I proceed in stages – trying blepharoplasty + brow lift + fat transfer first to see if I’m satisfied with that. I am skeptical this would give satisfactory results, but what are your thoughts? If we did something like this, would we still have the option of adding the implant later?
4. I feel unclear on some important details of the surgical plan, like where the incisions will be made, where the brow bone will be reduced, etc. Do you have an article or other description of these procedures that closely matches what you are planning in my case? Or how can I best get educated on these details? (I have been reading articles on the website, but don’t know how closely they apply to my case.)
A: In answer to your VOD questions:
1) The major risks are aesthetic in nature and mainly revolve around how well the eyelids follow the eye superiorly. In VOD perfect symmetry is rarely obtained, it is a question of the degree of improvement.
2) I have never yet experienced any significant complcations from this type of orbital surgery.
3) I can only comment on what I do. I can not speak for other surgeon’s experience or techniques. Certainly doing the procedures that have even mentioned can be done as they do not burn any bridges for doing other procedures later.
4) I would go to www.exploreplasticsurgery.com and search under vertical orbital dystopia where the procedure is fairly well explained, both in description and with pictures.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to know if the temporal constriction/reeduction is feasible. My forehead and the left and right sides of my skull above my ears are wide, which makes my head bulky in a beatle or tie. Maybe the temporalis muscle resection isn’t going to be as effective as I’d like. The hair transplant was done but made it look bigger. Is it possible to reduce the width of my upper skull by bone grinding or excision?My CT is attached to the file. Thank you very much.
A: Thank you for your inquiry and sending your pictures. The traditional temporal reduction procedure is done further back than you have illustrated, that is why it is called the posterior temporal reduction. You are illustrating an anterior temporal/bony temporal line/side of the forehead reduction…which can be done but requires a coronal scalp incision to do so. The key to the anterior procedure is the large amount of muscle thickness that has to be reduced and not the bine which is quite concave underneath it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it achievable via liposuction or removing of excess skin to get a uniform “smile” gluteal fold across both glutes. This problem has deeply affected my self esteem and i am looking for someone with experience in correcting the issue with beautiful results. Your response and considerations will be greatly appreciated.
A: Thank you for your inquiry and sending your picture. What you are seeking is to have a uniform infragluteal crease on both sides. Right now you have a partial double fold, a higher medial partial crease and a lower complete crease.
One can not liposuction between the two and create a single infragluteal crease. This is often tried but never works. Rather this requires an excisional approach where the skin is removed along the lines of the existing two creases and put together into a single crease. (lower buttock lift/tuck) Whether the resultant scar to do so would be viewed as a worthy tradeoff is patient dependent.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a lip lift done last year in which 11 mm of skin was removed from my philtrum, which was 24 mm, and I’m wondering if there are any procedures that could be done, for example tissue expansion or skin grafting, that could add some mm back to the philtrum.
I scar pretty well so I’m willing to risk a potential scar to restore the proportions and function of my face and philtrum.
A: There is no lip lift reversal procedure…short of a skin graft which would produce unacceptable scarring. This is why in a lip lift the amount of tissue removed should be cautiously done as there is going back. You can always do more but never can less be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a very serious facial problem, the left side is different from the right, and the left eye is smaller than the right and the mouth goes more to the left. Please let me know if you can perform surgical corection. Thank you
A: Thank you for your inquiry and sending your pictures. You have classic congenital facial asymmetry which is superiorly based which is why your lower eye/VOD is the most visible part of it. (VOD = vertical orbital dystopia = lower eye) The VOD can be effectively improved usng a 3D CT scan of the patient’s face to create a custom implant that raises the eye which also needs to be accompanied by upper and lower eyelid/eyebrow adjustments to go with it.
Correction of the VOD is the most significant way to untwist the face/lengthen the shorter side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read about your procedure to shave a Subcostal Rib Protrusion. I had a trauma to my left rib. After it fully healed there is a pointy protrusion that interferes with laying on my stomach or side on hard surfaces (like yoga, Jiu Jitsu, or even just crawling under a car to work on it).
Can you tell me how often you have done the surgery? Do you have any before and after photos? What is the recovery time? How bad is the scarring?
Thanks
A: I have done a handful of subcostal rib protrusion patients…all with the same history of trauma. Usually what occurs is a disarticulation of the costochondral junction with a resulting protrusion of the more mobile cartilage side. You are correct in that the protrusion can be be reduced by shaving of the cartilage to make it more level with the bony side. I would need to see a picture of the chest wall protrusion to confirm this supposition based on your description of it. The scarring from the surgery is very small as the surgery uses the ‘mobile window’ concept. There are no physical restrictions after the surgery as you can not harm the surgical site. There will be some expected soreness and it usually takes about a month until one can comfortably return to any form of strenuous physical activity.
Dr. Barry Eppley
Indianapolis, Indiana