Your Questions
Your Questions
Q: Dr. Eppley: I am planning to get cheekbone reduction and currently my biggest concern is skin sagging. But i already accepted the risk of skin sag i just want to minimize the severity. I read somewhere cheekbone reduction through coronal incision reduces the risk of skin sagging. Is it true? Which method is better?
A: It is true that the risk of soft tissue cheek sagging with a superior coronal incisional approach in cheekbone reduction osteotomies is less. This is because the stripping of the soft tissues off of the cheek coming from an inferior (below the cheekbones) intraoral incision is avoided. But there are adverse aesthetic consequences to the scalp approach as well, primarily the long scalp incision, the risk of visible scarring and the longer duration of the surgery which will increase the cost of surgery.
Ss you can see no approach to cheekbone reduction surgery is risk free. Your decision as to how to do cheekbone reduction surgery is based, therefore, or which risks you choose to accept if you have the surgery.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a cheek implant put in 25 years ago. Due to stress I have been grinding my teeth at night. I do wear a mouthguard. Twice over the past few months, I have woken up in pain where the implant is located. The first time I thought I had an infection in my gums and I took penecilin. It did go away but I was also very careful about managing the grinding. I just woke up 3 days ago with the same pain. I believe it is the implant and not a gum problem. I can’t even chew on that side it is too painful.
A: I believe what you are experiencing is a problem with your cheek implant. Undoubtably with such old cheek implants they are probably placed anteriorly with a downward angle, putting them close to the maxillary vestibule. Short of a tooth-related problem, which I can not say does not exist, the next culprit would be the cheek implant. The key question now in their management is whether implant removal alone is enough or whether replacement is desired.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in cheek implants hoping to eliminate the concave appearance of my cheeks and if possible strive for a more symmetrical appearance.I had cheek implants last year and think there’s plenty of room for improvement;).
Thank you for your time and I look forward to hearing from you.
A: Thank you for your inquiry and sending your pictures. The key to determining how to augment your cheeks better is to know what type of cheek implants you have in and where they are located. There is no sense in guessing or eyeballing how to improve things. That is why I would get a 3D CT scan which will reveal that valuable information. Once you know what isn’t working well it allows one to determine what will work better.
That is a scan we can order for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question. Is it possible to have a sliding genioplasty for the chin and create a custom wrap around jaw implant together. Reason I ask is that I think I need vertical length in my chin and it’s my understanding that chin implants only give horizontal lengthening.”
A: Combined sliding genioplasties with custom jawline implants are not uncommon. They are done when the desired chin augmentation dimensions, usually vertical, exceed what the soft tissue chin pad can safely cover. This usually is done when the combined vertical and horizontal augmentation dimensions exceed the combined number of 12.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I believe I may have excess perioral fat, and I am writing to enquire exactly what these pockets of fat around the highlighted area is.
I am situated in London England therefore I am asking to get an opinion on what exactly the right procedure could be. I have already had complete buccal fat removal however this treated my middle cheek and not the perioral area.
Could these be treated with an injection such as Kybella or would micro lipo be a more appropriate approach?
A: Kybella never works for fat reduction in that area, it requires liposuction alone or combined with a buccinator myectomy. In thinner faces it is most likely going to require both to create your outlined effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My concerns are that my sagittal ridge reduction will be sufficient enough. That there will be no long term affects from having it done. And that I can fly home the day after the surgery as I was told at my virtual consultation.
A: In answer to your questions:
1) In sagittal ridge reduction the maximum amount of height is reduced that the bone thickness will permit. Whether the line you have drawn can be achieved can only accurately be determined by a preoperative 2D CT scan to visualize and measure the bone thickness.
2) I am not aware of any long term effects from the procedure.
3) A drain is used and is removed the following day. One can go home thereafter.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I for two years I have been looking for a solution to my problem. I had a genioplasty (periosteal detachment of the mandible with milling of the chin bone relief with the pineapple ball). Since then, my chin is hyperdynamic (spasms all day long) and all the chin tissue is falling (including the mentalis muscle). It is very annoying and my chin is very long like a witch at rest and even more when I laugh. You can see my incivilities and I have to force my mouth shut. Here in France, the problem is little known. I have read your articles, you are an expert in this matter. Can my chin problem be totally corrected? I’m talking about aesthetically because my face is disfigured because of this witch’s chin and medically because I can’t even close my mouth and the spasms make me tired.
The first picture is me before genioplasty. Is it possible to get back the exact same chin I had before the surgery? Can surgery solve all my problems both aesthetically and functionally? Or is it complicated?… What do I have to do to remove the mentalis and the submental skin? I would like to get back the exact same chin I had before.
A: This is exactly what I would expect to happen from a poorly thought out chin reduction procedure. When you detach the soft tissue and reduce the bone support this creates the problem of soft tissue chin pad excess. The chin pad has virtually no ability to contract when the bone support is removed leading to chin ptosis, either at rest, smiling or both. As a result, the redundant soft tissues ball up and the mentalis muscle never works quite the same because it has lost its original working length.
Improvement is possible and the technique to do so depends on whether the chin bone is desired to be restored or not. If so I can consider an intraoral sliding genioplasty with muscle/chin pad resuspension. If not then a submental excision/tuck is needed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, , I’ve attached some pictures of my original nose before surgery and then some pictures of how my nostrils are shaped now after surgery due to the alar base reduction. I’ve labeled every single picture so that its clear which one is post op and pre op. I’ve also pointed out with arrows of how the nostrils have been brought down. One of the pictures is immediately post op in operating room.
I did not ask my surgeon to perform this procedure, and he did not give me any information on it prior to the surgery. He basically removed the alar base where I had the natural curvature of how my nose met with my cheeks. He brought the nostrils downwards and now it looks very weird and is causing my nose to look flat and wider than prior to surgery (since he has aligned it with my columella).
I know there are ways to reverse this with grafting but scarring is an issue. I wanted to show this to Dr. Eppley as I know he has a lot of expertise in reconstructive surgeries and may have methods to reverse this in a natural looking way.
A: You can not reverse alar base reduction surgery. Once skin is removed you can’t put it back without unnatural and very noticeable scarring.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, hey! i was looking to get a chin reduction, I have a wide and boxy chin, very prominent when I smile. how much would it cost to be able to fix it? I’ve heard it could cause jowls, how would that be avoided? thank you:)
A: A chin reduction does not necessarily cause actual jowling in my extensive chin reduction experience. But the best method to avoid ay chance of that is an intraoral approach through an osteotomy with midline resection which will make sure the tissues at the sides of the chin do not become adversely affected by maintaining their attachments to the bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about temporal reduction”
1. In regards to the convexity that starts above my ear, how much does the temporal bone contribute to the convexity, is the convexity all muscle whilst the temporal bone is straight. Please review my cat scans to confirm what my condition is.
2. Have you ever worked on patients where you removed/reduced the anterior section of the temporalis muscle as well as the posterior section and whether they had any post op complications such as jaw movement, lack of blood circulation with the scalp, hair loss etc?
3. How thick is the temporal bone, is there enough thickness to burr down the temporal line or the temporal bone itself 4. Based off the concept with form following function, considering how the temporal bone & temporal line had expanded due to the well developed temporalis muscles. Down the track after surgery, if I constantly wore a hat tight enough, not to the point of cutting circulation of course, can I reverse the growth and reduce the width of the bone?
A: In answer to your questions:
1) Both the muscle and the bone contribution to the width of the head above the ears. In most people, and you are no exception, they share equally in that effect. The difference in deciding to treat muscle, bone or both is really not what the contribution of the bone is. But whether one can accept an incision on the side of the head to do the bone burring. While muscle removal can be done with a hidden and virtually unfindable scar, the bone must be treated more directly and not from a remote hidden incision.
2) Anterior temporal muscle reduction can be done but it is done differently as it requires a direct incisional approach to do so. Whether it is done in conjunction with posterior muscle removal or by itself, it will definitely have a short term effect of restricting jaw movement in the early recovery period as the bulk of the working part of the muscle (70%) lies in the larger anterior section. I have done both together before but be aware of the short term jaw stiffness that will ensure by so doing.
3) In my observation and experience the thickness of the temporal bone does not allow for much reduction. The temporal bone is the thinnest of the external skull bones.
4) You will not reverse or change the shape of the temporal bone by compression. That only works in infants and very young children where the bones are still forming. But It will not affect the developed adult skull bone.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a genioplasty with you back in June. I am still happy with the results and everything healed up perfectly.
My face no longer looks “short” to me with my new chin, but I still think it looks too chubby for my BMI. My BMI is about 23%, I am comfortable at this weight and am not sure losing a ton of weight would even be healthy. I don’t feel the fat on my face matches my body/BMI. Maybe I am wrong and should try to lose a bit?
I am considering buccal fat removal and know you also do perioral liposuction. My face looks kind of “chipmunk” or even a little jowly to me. I wanted to ask him if he thinks I would be a good candidate for buccal fat removal or if I would need both buccal fat removal and perioral lipo or neither or something else. I attached a couple of recent pictures.
A: Thank you for the longer term followup. Many vertical chin lengthening patients actually do facial defatting (buccal lipectomies and perioral liposuction) procedures either concurrently with the chin or before or after the chin. So your request and goals is not atypical and the dual bone lengthening and fat removal procedures are synergestic.
Both adjacent midfacial fat locations are of benefit for treatment and usually the lower cheek fat (perioral liposuction) adds as much to it as the buccal fat even though its total volume reduction is less. (as it is closer to where the chubbiness look is the greatest.
Fortunately these cheek reduction procedures are a lot easier to go through with less recovery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Since I was about 15 I have had this bony growth around upper orbit and brow bone on the left side. It is quite noticeable, and I think it has pushed my left eyebrow down and caused one eye to appear “swollen” – there is a lot of extra skin above upper eyelid compared to right side. Was scanned and was found to be benign, cause unknown and no specific incident of trauma comes to mind as to what could cause it. Curious about the procedure in shaving down/reconstruction if necessary, if its the result of some sinus asymmetry or if the bone lies on top of the thin brow bone. Also curious about costs, recovery time, side effects and tradeoffs of surgery.
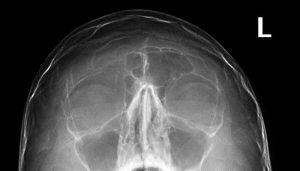 A: What you have, as is evident in your plain skull films, is an over pneumatized (overgrown) left frontal sinus. It is benign and why it has so occurred will never be known. What what is known is that in trying to treat it shaving or burring it down is absolutely what should not be done. The overlying bone is too thin to do so. This requires a bone flap setback technique. This is where the overlying bone is removed, reshaped and put back which makes it less protrusive and more normal in appearance.
A: What you have, as is evident in your plain skull films, is an over pneumatized (overgrown) left frontal sinus. It is benign and why it has so occurred will never be known. What what is known is that in trying to treat it shaving or burring it down is absolutely what should not be done. The overlying bone is too thin to do so. This requires a bone flap setback technique. This is where the overlying bone is removed, reshaped and put back which makes it less protrusive and more normal in appearance.
The major consideration in this form of brow bone reduction for men is the incision to do the procedure and the resultant scar. This has to be done through a scalp incision located either at the frontal hairline or behind it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello I’ve spoken to your office a few times and was wondering if getting a custom wrap around jaw implant and sliding genioplasty with some kind of lower/neck lift could all be performed at the same time.
Thank you
A: The question is not whether you can have a jaw implant, sliding geniopasty and necklift at the same time but whether you would really need all three. Total jawline augmentation often provides a neck lifting effect that may obviate the need for a formal necklift.
But to provide a qualified answer I would need to see some current picture.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a lumpectomy and radiation on my right breast in 2013. I would like to have a breast lift and implants. Will radiation prevent me from being able to have surgery?
A: Your question is very appropriate as radiation changes the quality of the tissues in its path and their ability to heal in addition to dramatically increases the risks of implant-related complications, (e.g., infection, capsular contracture) So jumping in and doing a breast lift and implant would likely lead to a high rate of complications.
In radiated tissues the key is to change the quality of the tissues by initial fat injections before doing any invasive surgery. Such fat injections are done three months before any aesthetic breast surgery is undertaken.
These are general principles in irradiated tissues and how they may specifically apply to your breast needs requires a picture assessment of your current breast shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, What is the height of the deltoid implant (the width that it adds to each shoulder)? Are there different sizes? Please kindly advise before I schedule a consultation.
 A: Since deltoid implants are custom made for each patient (there are no true standard deltoid implants) their width can be made to what the patient wants….provided that it will fit. (which is my call)
A: Since deltoid implants are custom made for each patient (there are no true standard deltoid implants) their width can be made to what the patient wants….provided that it will fit. (which is my call)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read that your office offers skull implants to grow an inch or so in height. I was wondering if it is safe for the implant to remain permanently and if it is okay to resume contact sports (football / kickboxing) after this procedure.
A: Skull implants, once placed, are permanent and, as an unintended purpose, actually acts a bumper on the skull adding a layer of protection. So participation in sports remains possible after having a skull implant placed. There are no known long term adverse effects from an indwelling skull implant that are known at this time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have discussed in the past regarding his thoughts on whether orthognathic surgery could also be done in my case. While my bite is not far enough apart at this point (partly because my lower teeth have developed an forward angle to compensate) , I am considering potentially have my lower teeth replaced with an implant supported prosthesis (all on 4 or 6) at the advice of a prosthodontist due to the condition of those teeth and he seemed to indicate that could make it possible to have my lower jaw advanced. I’d really like to get your opinion on whether you feel this is a possibility (as it’s a procedure we’ve again discussed previously by e-mail). I really feel like advancing my lower jaw would provide further aesthetic benefit (while the jawline/chin implant certainly has helped in this regard, I still feel like my short lower jaw is noticeable — at least to me) and perhaps addressing it could even improve my sleep apnea as well. If he feels it is a possibility, is this a procedure that you perform (I am almost certain I’ve read where you have done it in the past but not really mentioned on the site) and if so, is it something that can be done potentially outpatient? I believe you had indicated to me in the past that it could be if only one jaw is involved.
A: The key question in orthognathic (jaw) surgery is the patient’s bite. Jaws are moved so that the teeth interdigitate better, thus there has to be a ‘malocculsion’ induced beforehand by orthodontic manipulations. Whether that can be done given your current bite relationship and what those movements would be requires an orthodontic evaluation since they are the ones that would be making those movements so they are in the best position to judge what is possible.
I would also bear in mind that with an indwelling jawline implant doing a lower jaw advancement would require its removal…so I doubt given the effort that has been put into getting it there that is infection free and in good position would be worth undoing it. It is probably better to just ponder increasing the amount of chin augmentation (which is only what lower jaw advancement would accomplish anyway) by either only chin augmentation or moving the chin bone forward with the implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am asking about breast reduction surgery for my overweight friend. She has a BMI of 43. Is it possible for her to get this surgery without losing weight? Her breasts are very large and saggy and cause her back and shoulder pain. She is much less concerned with aesthetics than she is in relief.
A: There would be no reason why one would need to lose weight before a breast reduction surgery, particularly when one has significant musculoskeletal symptoms. Yes it is more ideal to be at a better weight before the surgery if possible but that is not an absolute exclusion criteria.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible for the nose to be vertically lengthened, giving a philtrum – shortening effect similar to a lip lift?
A: Your question is really whether a ‘reverse lift lift’ can be done where the nasal base moves downward instead of the upper lip moving up with a subnasal base tissue excision. In general no as the nose is a more fixed structure while the upper lip is not and is very mobile. With the one caveat that the base of the nostrils and the base of the columella can be moved downward a few millimeters…the operative term a ‘few millimeters’ being the key phrase.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering if the doctor does permanent lip filler removal? I’ll also need another procedure to give them shape and volume again.
A: Permanent lip filler, which are most commonly of silicone materials, have to be removed by an open procedure. Reshaping often involves changing the level/position of the vermilion border. The placement of solid fat grafts is usually what is done as the silicone material replacement since an open space has been created by the excision of the material.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am past 6 weeks since my second tummy tuck. I can see a difference however, it is not anywhere near what I was hoping for. I can still grab a hand-full of fat all around my abdomen, my measurements have not reduced at all and I still feel swollen on the inside however, the skin feels normal softness on the outside. I am very concerned because this is the second tummy tuck I have had with this surgeon as the first one left me worse off than my natural body so revision surgery was performed. The scarring is better this time and at least I can see results however, where I am now, is not much better than my natural, pre-opp body. The photo is my pre-opp body but 12 months after TT 1 and 4 weeks after TT2. I am now more than 6 weeks post opp and don’t feel any different from 4 weeks. What can i do to reduce the swelling? I am very concerned that I have been through the procedure twice and for all losses and no gain.
A: Thank you for your inquiry and sending your pictures to which I can make the following comments:
1) For having had two tummy tucks I would agree that the change is far less than expected.
2) What is not clear is what exactly was done in these two procedures. The term ‘tummy tuck’ is a generic one and does not specify as to the particulars of the procedure. I suspect yours was more of a mini tummy tuck and I see no evdience of liposuction of the entire abdominal and flanks areas being done concurrently. But in fairness to all involved without reading the operative notes from the procedure and seeing the actual scar location I can only speculate.
3) What is not speculative, however, is that what you see now is probably more of the actual result than reflective of an overall swelling effect.
Dr. Barry Eppley
Indianapolis, Indiana
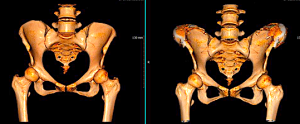
Q: Dr. Eppley, Hello, I am just inquiring if you are able to correct SCAPHOCEPHALY, which is when the head shape is slightly narrow and abnormally long?
If so, are you able to help children and adults?
Thank you
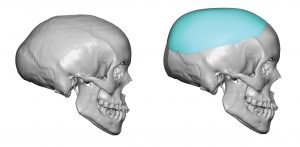
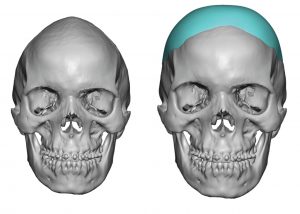 A:I do have an approach to treat adult scaphycephaly as seen in the attachments which consists of some anteroposterior bone reduction and widening skull implant augmentation.
A:I do have an approach to treat adult scaphycephaly as seen in the attachments which consists of some anteroposterior bone reduction and widening skull implant augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi Dr, will I be able to move and rotate my shoulders and hands freely after clavicle shortening? And will I be able to play some simple hand sports?
And, is there a plastic surgery that can increase the vertical length of my chin? My chin is so small and short and my face looks like a baby because of it!
A: In answer to your questions:
1) When fully healed from clavicle shortening surgery, normal arm range of motion will be present as well as the ability to play sports.
2) You are referring to vertical chin lengthening through an opening wedge genioplasty. Up to 10 to 12 mm of vertical chin lengthening cvan be achieved.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I was wondering whether anterior and posterior temporal muscle reduction and temporal bone reduction can all be done in the same day, I know you prefer muscle reduction than bone reduction but are you able to have both done in the same day
A:It is not that I ‘prefer’ temporal muscle reduction for head widening reduction, it is just that bone reduction achieves so little (the temporal bone is very thin) and requires a direct incision on the side of the head to do it. Thus it adds little to the final head narrowing effect. This is why it is very rarely done in my experience.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, First off, thanks for being a pioneer in this field and paving the way for other surgeons to follow suit. My question is with regards to your blog: widening vs vertical jaw angle implants. In it you say, a widening implant can add a little bit of vertical dimension as well. How much realistically achievable in vertical height? Would 3-4mm be realistic (depending on positioning) and how is this achieved purely by adjusting positioning?
Thank you so much in advance and with regards,
A: I would say that a visible 3 to 4mms of vertical lengthening is seen in the proper placement of widening jaw angle implants due to the soft tissue roll effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I did have a small size chin implant inserted several years ago which I am very happy with. I think a larger one would leave me with a boxy chin. I do not want to try to look younger either. But I do feel I have a somewhat weak lower facial profile and I wish it were otherwise.
I had the thought that bringing the lower jaw forward a little and slight lengthening of the lower face could be a solution but I am unsure. I do not think a larger chin implant by itself will provide the answer. I have read many on articles on your website and on Real Self online. As example, “What Can Be Done To Give My Face More Of A Sculpted Masculine Look?” “What procedures could I do to make my face more masculine (low straight eyebrows, defined jawline and chin)?” “The Vertical Lengthening Custom Jawline Implant – Making the Lower Face Longer.” I have a lot of respect for your expertise and aesthetic eye in these matters which is why I contacted you to arrange a consultation.
I do feel a stronger profile would help. And a face with stronger features is an investment I am very interested in. What procedures would you suggest I do to obtain this stronger profile and perhaps more handsome appearance.
A: Thank you for your inquiry and sending all of your pictures as well as congratulations in finding that second career. You are correct in that in the congenitally smaller lower jaw a modest chin implant provides improvement and looks natural. However when a larger chin implant is placed it becomes out of proportion to the small jawjine behind it and looks unnatural. Thus enlarging the whole lower face through total jaw augmentation is an appropriate consideration. The key to total jaw augmentation is still not to go too large and I have attached what I would consider one version of a reasonable jaw augmentation effect. One of the side benefits of total jaw augmentation in the older male is that it picks up loose skin in the neck and with the more evident transition between the face and neck (more visible jawline) a bit of a necklift is achieved as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering about follow-up to https://exploreplasticsurgery.com/plastic-surgery-case-study-outcome-assessment-of-transgender-male-to-female-shoulder-narrowing-surgery/?doing_wp_cron=1633484309.4748740196228027343750
Specifically,I was wondering if you had any photos showing a back view after the patient had time to recover from the surgery? In the “1 day after” photos, the patient appears to have extremely hunched posture which looks to compromise the aesthetics.
A: As stated in that case study, every shoulder narrowing patient in the first few weeks after surgery will have a hunched appearance as that is the most comfortable position to protect the healing clavicles. That is not a long term shoulder appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, As a trans woman considering iliac crest implants does one need to be on hormones prior to the surgery?
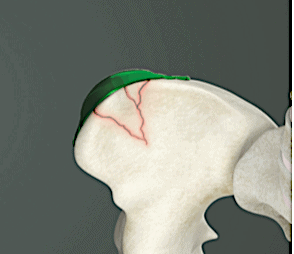 A: While many transgender women are on hormone therapy, and I would consider this to be the normal, it does not have a beneficial or adverse role in successful implantation onto the iliac crest. Good healing ix expected whether one is or is not on hormone therapy.
A: While many transgender women are on hormone therapy, and I would consider this to be the normal, it does not have a beneficial or adverse role in successful implantation onto the iliac crest. Good healing ix expected whether one is or is not on hormone therapy.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, what is the recovery time for iliac crest implants?
 A: The recovery time from iliac crest implants is a direct reflection of having raised part of the TFL fascia off of the iliac crest to place the implants. This causes some discomfort with walking as would be expected initially. This will take several weeks to fully resolve so exercise is going to be delayed for a month or so after the surgery. There often is some numbness in the front of the thigh but this will usually subside within months after the surgery.
A: The recovery time from iliac crest implants is a direct reflection of having raised part of the TFL fascia off of the iliac crest to place the implants. This causes some discomfort with walking as would be expected initially. This will take several weeks to fully resolve so exercise is going to be delayed for a month or so after the surgery. There often is some numbness in the front of the thigh but this will usually subside within months after the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley: I weigh 375lbs highest weight was 400. I am trying so hard to loose weight but my “fat appron” is causing a lot of issues for me. Rubbing raw and so painful when I try to exercise. I feel I hit a wall. I really want to get a panniculectomy and was curious if this could be done at my weight. I need it gone to continue my weight loss journey!
A: Thank you for your inquiry and sending your picture. I believe you are correct in that only a removal of the double/triple roll abdominal tissue excess can provide the psychological, and perhaps physical, springboard for continuing on your weight loss process. I have seen this many times and, although classic teaching is that weight loss should be first maximized before surgery, that is often not effective and many patients like yourself hit the proverbial wall. Such surgery provides very positive feedback so the patient’s motivation for further body reduction efforts is reignited.
Unfortunately I will be unable to help you as my surgery center has a patient weight limit of 300lbs due to the beds that we use. At such a weight the surgery will have to be preformed in a hospital where they have operative tables that are made for such patient weights.
Dr Barry Eppley
Indianapolis, Indiana