Your Questions
Your Questions
Q: Dr. Eppley,I would like to undergo the surgery for brow bone implant augmentation, and I am wondering what the sequence of steps will be. I live in Southern Washington, so I assume that I would need to travel to Indiana for the consultation, CT scan, and the surgery itself. I recently learned that there is another type of implant material, porous polypropylene, in addition to the standard silicone material. Do you use this type of alternative material?
A: In answer to your brow bone augmentation questions:
1) the needed 3D CT scan is one you get where you live. We help you find a place to get it and then place the order so you can have it done. Then you mail the disc to us.
2) All consultations, discussions and implant design sessions are done online. You only come here once for the surgery.
3) Porous polyethylene, also known as Medpor, is another facial implant material option, But it offers no advantages, has numerous disadvantages and adds considerable cost to the surgery. i only use it when that is what a patient wants.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, After my sliding genioplasty my bottom lip is stuck down and can’t move up all the way. What can I do to fix it?
A: While one side view picture provides limited information, a likely cause is that the vestibule on the inside of the lower lip is contracted down into the bony stepoff that has been created by the bony genioplasty. A side view x-ray and a lip pull test would conform that diagnosis. If so the vestibule needs to be released and the bony stepoff grafted, usually with a dermal-fat graft, to provide improved lower lip mobility.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Will I be able to take hard hits to the head and will my hair grow back again after skull reduction?
A: Skull reduction surgery does not affect hair growth. It also still allows adequate brain protection against traumatic injury.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a facelift 3 years ago which left my right tragus blunted. I am self conscious about it’s appearance and never wear my hair up in public.I see that you have experience with this type of deformity.
A: The blunting of the tragus from a retrotragal facelift is due to scar contracture on the tragal cartilage pulling it forward. Technically the problem is a skin shortage and a cartilage deformity. What usually effectively treats it is a release (raising a skin flap over it), rebending and suturing the cartilage back and then advancing the skin flap back over it. (ideally a small full thickness skin graft is most ideal but you don’t want to create a skin color mismatch over it)
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a question that I wanted to see if you could address. I previously had a alar base reduction and am devastated with the results. The surgeon removed 2.5mm but even that little amount made a big difference as it changed my nostril curvature.
I have been suggested by another doctor that an option is to take a small piece of skin from my nasal floor (where the alar base reduction should have been done originally to avoid losing the curvature) and place that piece of skin into the curve. The skin is the exact same color and contour so irregularities will not be a problem. The second option is taking a small piece from the bottom of my nasal rim (my nostrils have been brought down so I need to have my alar rim raised anyways). My only question is regarding stitching. Since skin is being placed back, I’ll have another marking of scar. Do scars easily fade away and are they noticeable?
A: The best advice I can give you is to be very careful when embarking on a corrective procedure that is also going to leave a scar of some sort. What you don’t want to do is in the goal of correcting one problem you merely create another new problem. In other words every procedure has tradeoffs. If you fix the nostril narrowing but end up with visible scarring, even if it is slight, is that a worthy tradeoff? I can not answer that question for you, only you can. But what I do know is there is no corrective procedure which will not have a tradeoff.
Be very careful about ending up merely going down the ‘rabbit hole’. Plastic surgery is littered with many rabbit hole patients…I see them all the time.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I desired a change for awhile but was too young. Have uploaded 3 images of me and 1 with a crude iPhone edit of what the end goal might be. Was mostly wanting to know how plausible it would be or if the desired results in my case are probably too much or too drastic. Essentially my main concerns are about the forehead. One being how it slants back starting right above the eyebrows, whereas I would like it to be more straight up and down. The second concern being that the top of the forehead is too low. The back of my head is at a higher peak than the front, I believe a more level top of the head front to back would look better for me in my case. The photo I crudely drew on just imitates what that might look like if the forehead was different in these two magnitudes. I know you are the best and would be using y’all if I did anything like this. If there are limitations that would prevent that much volume being added it’s just something I’ll have to accept lol! Thanks so much for taking the time!
A: Thank you for your inquiry, detailing your concerns and sending your pictures. Your pictures are taken from fairly far away so I enlarged them and laid them out side by side to see your imaged changes. You are correct in that the near vertical inclination of the forehead is a bit much…for a reason that is not apparent in a side view picture. When you add that much volume in the forehead in profile you have to consider the effects in the front view as well. Since the forehead like the rest of the skull is a large convex surface you can’t just add volume in one dimension without doing so in all other surface dimensions. In other words as the forehead inclination becomes less (more vertical) it must also become wider or the forehead will just look like a porpoise. As a result there are some aesthetic limitations and also some volume limitations based on the stretch of the scalp. Thus the best way to visualize what could be done is to assume that the achievable aesthetic outcome is probably halfway between your ideal and the shape of the forehead you have now.
Dr. Barry Eppley
Indianapolis, Indiana
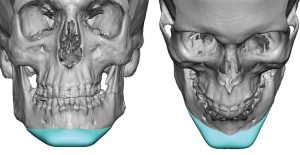
Q: Dr. Eppley, I am interested in Maxillofacial Surgery, specifically jaw repositioning (jaw advancement). I have an underbite. I clench my jaw and have TMJ. I want to advance my jaw so that the top and bottom set of teeth are aligned evenly. I like the aesthetic look of an aligned top and bottom jaw. I also like the ease of tension from constantly biting down. I would like to know if its possible to insert and orthopedic plate somewhere on my face bones to prevent my jaw from moving back and to encourage it to rest in the new, forward position. I want my jaw to still be able to move up and down and forward, but not back. Moving back serves no purpose & I don’t like a weak jaw profile at all. I have inserted a photo to explain what I mean by ‘new jaw position’. Please let me know if this is possible. If not, is there another way to achieve this look? Or is this purely dental work? I appreciate your time. Thanks.
A: What you are referring to is the common operation known as a sagittal split mandibular advancement. (SSRO) This requires preoperatve orthodontics in preparation for the surgery. The place to start is with a local orthodontist whom you can work with and they will coordinate that with a local surgeon who can do the actual surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am wondering about artery ligation, I have an artery that pulsates and is bulging, I don’t believe this is from the temporal area ,it is above my left eye and goes into my scalp. (pictures attached) Over the last 2 years it has become more prominent, I’m wondering if it’s possible to ligate this artery safely to reduce or eliminate the appearance, I have been checked for temporal arthritis prior with negative results.
Thank you very much
A: The central forehead is a very unusual place for a prominent artery to appear. The vast majority of prominent facial arteries comes from a branch of the superficial temporal artery at the side of the temples/forehead. Most central prominent vessels are larger and are veins. in rare instances it may be the branch of the supraorbital artery (which appears to the case in you) which comes out of a foramen in the brow bone and courses upward across the forehead into the scalp.
To ligate the supraorbital artery this requires a small incision inside the eyebrow to ligate the proximal point (forward flow) and then another small incision behind the frontal hairline to llgate the distal point. (backflow)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need your opinion on what would help me best (even if you won’t perform it) on a rib procedure I am looking to get done. I’ve read so much about you and am just really amazed at the unique work you do and the number of lives you’ve changed. anyway here is my issue. I was born an identical quadruplet, and as a result I was given some congential problems that has destroyed my confidence in my body. So I have assymetrical ribs. And by this I mean there is a thinner side (the right) and a thicker, protruding side which is the left (this is also reflected in my chest wall, my left pec easily grows thick while my right does not). My problem is, not only is it very unappealing, but as I work my abdominals, the thicker side gets all the work and those abs get overdeveloped. What am I wondering is what would be the best way to get the thicker side rib cage in the subcostal region (where the upper abdominals are shaped) to match the thinner, flat side, so my abs can be at a symmetrical level and my stomach be more symmetrical and thinner. I’ve attached a few photos as an example. I am a very motivated patient, and would do anything to get the left ribs to be flatter and as thin as the right. What would you suggest I tell a qualified surgeon to do? I really really appreciate you and all the knowledge i’ve gotten from you and read on your site. You give me hope that my body won’t always be a point of such deep frustration. Thank you.
A; Thank you for your inquiry and sending your pictures. What you have is an ipsilateral protrusion of the right subcostal cartilaginous ribcage. It is probably not that the subcostal ribs are ‘thicker’ but the arc or curve of the ribs is greater than that of the opposite side. A 3D CT scan of your ribcage would confirm the exact anatomic anomaly.
The question is not whether this subcostal rib protusion can be reduced, as it can, but how to do so with the least amount of scarring as possible. Such subcostal rib protrusions are reduced, usually by shaving, through direct incisional access with an incisional length of 3 to 4 cms.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had dermal fillers to the tear troughs and cheeks three months after having brow bone implants. How likely is it for the implants to get infected because of the injections? Will the capsule around the implant prevent the infection or the capsule hasn’t formed yet?
A: Injectable fillers placed into the cheeks and tear troughs are not going to migrate superiorly up to the brow bone area. Thus I would say the chances of getting brow bone implants infected from cheek injections would not be very likely.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an inquiry regarding forehead asymmetry. My right frontal eminence is larger than the left, I am unsure if it is due to natural asymmetry or perhaps from mild unicoronal crainiosynotosis. The left side has less projection and is generally flatter, which continues to the coronal ridge. I had a CT scan done a few years ago, which I unfortunately have had trouble locating recently. I am curious to the extent a unilateral custom implant could improve the symmetry of such a case. I recognize an issue in such an implant would be visible implant borders along the forehead.
Any feedback would be appreciated, and thank you for your time today.
A: Using a 3D CT scan a unilateral custom forehead implant can be designed to improve your forehead symmetry. With the feather edging of the forehead implant having a visible edge of the implant on the forehead, while a potential risk, is not something I have yet seen.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am inquiring about to possibilities surrounding your clavicle lengthening Q: Dr. Eppley, I am inquiring about to possibilities surrounding your clavicle lengthening procedure. I understand that you have two techniques for lengthening the bone, one being an oblique cut into the bone and the other a sagittal split pattern. I was hoping if you could tell me which one is able to extend the bone the longest.
A: The sagittal split osteotomy pattern allows the clavicle to be lengthened the most…but still should not be more than 2.5cms per side to ensure that adequate bone healing takes place.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking into shoulder reduction surgery, and also breast reduction and rhinoplasty. I am from the UK, so if I was to travel to your practice to have these surgeries, would it be possible to have them done at the same time?
A: Thank you for your inquiry and detailing your surgical objectives. Shoulder narrowing, breast reduction and rhinoplasty could all be done in the same surgery. The controlling factor in the recovery would be shoulder narrowing…breast reduction and rhinoplasty do not create much discomfort and are less limiting than shoulder narrowing in the recovery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have mild/moderate plagiocephaly for which I intend to try and surgically correct as much as possible in the near future.
As you can see from the attached photos, the right side of my skull is prominent by several millimeters / 1/4 inch with a corresponding flat area on the back right of my skull. My jaw (and to an extent my whole face) is skewed to the recessive left side.
What is your opinion of the success of treatment options.
A: Thank you for your inquiry and sending your pictures. You have the classic plagiocephalic skull and facial changes which only differ in affected patients by their magnitude. I always use a 3D craniofacial CT scan to treatment plan. But in the end you treat what bothers patients by what they see externally. Also as part of the treatment plan the goal is also not to create undue scarring from the surgery.
That being said you have identified one very definitive concern, the flat back of the head on the right side and the ipsilateral protrusion of the parieto-temporal bone to which my treatment approach is a custom skull implant to build out the flat skull area and an ipsilateral temporal reduction to reduce the width through an incision in the crease in the back of the ear. Both are very low scarring procedures that are highly successful in improving the head shape to most patient’s satisfaction.
The facial asymmetries are a bit different in that they are more subtle and I would have to defer until seeing a 3D CT scan to make any treatment recommendations. In addition I need input from the patient as to those concerns, particularly what they see as the most bothersome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I just want a harmonization from my lower face. I think my lower cheeks are too fully and my upper and lower jaw are to small. I feel it because i bite on my tongue and you see on the pics my teeth are going forward.
Additionally i bite really often on the inside of my cheeks
Anyway, i thought to solve this all it is important to go to a specialist. He can see what procedure came with the best results…So maybe you have some good ideas for my problem.
You can see on my pics how it is and how i imagine it.
I would very much look forward to a personal interview!
A: Thank you for sending your imaged/wish pictures. What you are demonstrating is a forward and elongation of your jawline with the jaw thrust maneuver. This can be achieved three different ways aesthetically and only one way functionally. (bite improvement) There are:
1) Orthodontics combined with entire lower jaw advancement (aesthetic and functional improvement) with sagittal split ramus osteotomy.
2) Vertical Lengthening Bony Genioplasty (aesthetic improvement of chin area only, no functional improvement)
3) Chin wing osteotomy (aesthetic improvement of chin and anterior 2/3s of jawline, no functional improvement)
4) Custom jawline implant (aesthetic improvement of entire jawline, no functional improvement)
The key decision points are:
1) do you want the bite improved or can it be left alone as long as the aesthetic objectives are improved?
2) If no change in the bite is acceptable then it becomes a question of whether wants to use only their own bone to achieve the effects or is an implant acceptable?
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in temporal implants. I have been getting injectable fillers into my temple for some time but am getting tired of the repeated injections and the cost. Do I have to dissolve the injectable fillers before getting temporal implants? What type of temporal implants do I need?
A: In answer to your temporal implant questions:
1) There is no issue with filler in the temporal region for placing an implant provided it does not interfere with the aesthetic assessment of how to design an implant to augment it.
2) Most hyaluronic-based fillers significantly or completely resorb in six months after their placement.
3) I assume you mean a custom temporal implant for one side? What temporal area is being augmented? Seeing a outline of the desired temporal augmentation zone would be helpful to determine the type of implant needed as well as determining the cost of the surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m considering getting a temporal skull reshaping. I have a narrow skull, and i want to know if i can make a widening along the sides of my head. I’m thinking like 2-3 mm on each side, I want it to look as natural as possible and not something you would notice so much. I live in Europe and would like to ask some questions before planning a trip to the US.
I know there are different methods, depending on how much needs to be made.
– Will a temporal skull widening with only 2-3 mm require an implant or can it be done with injection using fat or PMMA/bone cement? I’m trying to avoid a heavy surgery.
– Is injection permanent?
– Will it affect my hair growth?
– How many cuts will there be and where do you place them?
– How much will it cost for a temporal augmentation like the one i described?
A: In answer to your temporal (side of the head) augmentation questions:
1) There is only one effective way to achieve a smooth augmentation over a large surface area like the side of the head regardless of its thickness…a custom temporal implant. Bone cements can only be used on bone not soft tissue like fascia or muscle. And even if they could they would have many irregularities.
2) No method of skull augmentation at any location affects hair growth.
3) A custom head widening implant is placed through an incision in the crease of the back of the ear.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a 30 year old male, I got an intraoral chin implant about 3 months ago to have a square shape and elongate my face a little. Unfortunately, It gave me more of a V shape to my face and I am not happy with the result. I was looking for a square masculine chin look.
Also I believe the implant was either misplaced or inserted too high as it made my lower lip thin and the area became very tight and uncomfortable.
I am looking to see if you can help me achieve this square look and also replace my existing implant.
A: While I don’t know what type of chin implant was used but if it achieved a V shape then it clearly was not a square style chin implant and had no chance to create that desired effect. Secondly the intraoral placement method would be exactly what you would not do if one of the chin augmentation goals was also to elongate the chin. This is very difficult to do intraorally unless one is very experienced at doing so, requires a specific type to do it and always needs screw fixation.
What you appear to have is an incorrect chin implant shape, was not positioned low enough and was never screwed in. This accounts for all of the symptoms that you describe.
What you know now is the following: 1) a submental implant placement method is needed for both removal of the existing implant as well as replacement with a new one and 2) a different style of chin implant is needed. Whether this should be a standard or custom chin implant design is open for discussion.
The two pieces of information that would be critical moving forward is some current non-smiling pictures of your face and 3D cone beam scan of your chin so we know exactly the shape and position of your current chin implant for my assessment. That information allows the following statement to then apply….’When you know precisely what doesn’t work well you then you know how to change it to be better.’
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My chest look amazing after getting pectoral implants, thank you. In thinking about my next surgery I have two questions: 1) can you do the biceps, triceps, and traps in one operation so I don’t have to go under twice? 2) During the operation can you also give me a cleft chin? Thanks!
A: Thank you for the followup on your pectoral implants and that is good news. In answer to your questions:
1) Bicep, tricep and deltoid implants can be done at the same time. One could argue that is probably not the best combination from a recovery standpoint. (it makes it tough with the entire upper arm has been traumatized) But understandably it is the most efficient way to do it.
2) Making a chin cleft, which are vertical in orientation and located on the lower half of the chin, are done by a soft tissue reduction method. That can be done through either a submental approach or a direct excisional technique. Which one is best depends on how deep one wants the chin cleft to be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have what I consider a receded chin, and I don’t care about anyone else’s opinion on it to be blunt. I want a more forward appearing lower jaw, and would like to get reconstructive jaw surgery, but if sliding genioplasty can create the profile I’m looking, then I would be willing to a less invasive surgery. My main concern with just genioplasty is the labiomental groove. Mine already bothers me a lot, and I need it to be much, much flatter. I’m also interested in Rhinoplasty but my main concern is my chin. I’ve attached a few pictures or my profile, as well as two edited photos to give you an idea of what I’m looking for.
A: When you a short chin, deep labiomental fold and lower lip eversion this is all a reflection of an overall short lower. What really improves the depth of the labiomental fold and the lower lip eversion is having the whole lower jaw come forward. As the lower teeth move forward this pushes the labiomental fold and the lower lip forward. Thus you ideally need a BSSO mandibular advancement…but it will not create by itself the chi projection you are showing. It would need to be combined with a sliding genioplasty also moving the lower jaw forward will not create that degree of chin projection.
The alternative to total lower jaw advancement is a sliding genioplasty combined with grafting of the bony stepoff with fat injections to the labiomental fold. This will not produce as good as a result of the labiomental fold correction as the combined lower jaw advancement and sliding genioplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would getting an implant on the back off the head, to correct flatness cause my hair to look really thin or weird, since the scalp would be stretched out?
A: That is a very good question and the answer is no. The scalp is not stretched enough to visibly increase the infrafollicular distances. It is important to differentiate the more limited scalp stretch that occurs from skull implants from that of what happens in scalp tissue expanders.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 3 years ago I had an endoscopic brow lift. I didn’t like my hairline to be elevated so 2 years later I had a reversal done, with the same method. The surgeon released the forehead by making 2 incisions hidden in the hairline. But the surgery failed as my hairline is in the same position.
Would a second surgery help to bring my hairline and brows back down ? And why can’t it be entirely successful ? If it is possible to bring the hairline up, it should be possible to bring it back down?
Thank you for your time
A:What is not obvious in an endoscopic browlift is the extent of subperiosteal tissue release that is done underneath those two incisions. An endoscopic browlift reversal is possible but the key is that the entire scalp must be mobilized and then secured in a more forward position. It is very similar to that of a frontal hairline advancement…minus the frontal hairline incision. In short you had inadequate scalp mobilization and lack of any means of soft tissue fixation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve lost around 40-50 lbs in the last year and a half and I have a lot of loose skin around my abdomen. Friends of mine who have helped me with my workout and nutrition routines recommended that I consult with you.
A: Thank you for your inquiry and sending your picture. Congratulations in your successful weight loss. You have the classic near circumferential waistline skin excess that typically develops after such weight loss. This is treated by a near circumferential tummy tuck also known as a belt lipectomy in older terms. Whether this needs to completely wrap around your waistline or only partially so remains to be determined.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wanting to get more information on shoulder reduction surgery. I want reduction on both shoulders however I have a previous injury on my left shoulder and still have a plate with screws there. Is this procedure still possible for me? Are there any complications my earlier injury will cause?
A: Thank you for your thoughtful question. It would depend where on the clavicle the plate lies, whether it would be in the zone of the osteotomy or not. Do you have an x-ray of that shoulder which shows the plate position? If the plate is in the zone of the osteotomy it can be removed and the clavicle reduction osteotomy done at the same time.
Dr Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Will I be able to take hard hits to the head and will my hair grow back again after skull reduction?
A: Skull reduction surgery does not affect hair growth. It also still allows adequate brain protection against traumatic injury.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have the following questions about custom brow bone implants, to make my forehead more masculine:
1. How soon after the surgery can I fly back home?
2. How soon can I return to work in a office-setting?
Thanks in advance.
A: In answer to your brow bone implant questions:
1) You could fly home the next day.
2) Returning to work would depend on how you feel about any swelling that persists in the recovery phase. Your restrictions after surgery are not physical but appearance related.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,I am male that has suffered from undescended testicles in the past. When I was a child, a surgery was performed. The result were very suboptimal. As a result of the surgery, my right ball is on the smallish side. My left testicle is less than 1cc in size and is stuck in scar tissue. The right testicle is between 3 and 4 cm in size.I had varicoceles reduction surgery years ago that did not help at all in terms of size. Adding insult to injury, my testicles have further shrunk since I started my HRT.
Several years ago I had a cosmetic surgeon inject my scrotum with 250 cc of a solution that has 1/3 of its volume in silicone oil. My body has produced close to 200cc in collagen (in addition to the 80cc of silicone). While I am happy with the size of my scrotum, I am very unhappy with my shape. I would like to research and consider the use of the testicular implants.
My questions:
1- I anticipate that I would need to remove a good portion of the silicone/collagen I have prior to the implantation of new testicles – can you do this?
2- I suspect that that I will need one side-by-side and one wrap around implant (what do you think?) and
3- How big do the implants get? (dimensions and volume) – I definitely like the idea of a testicle size in excess of 80cc – maybe significantly more.
A: Thank you for your inquiry and sending your pictures. This is obviously a novel situation when it comes to testicle implants. (at least I have not seen it before) In answer to your questions:
1) I do not see that trying to excise the silicone/scar tissue conglomerate would be recommended. That will create a host of new problems including scarring, tissue contraction, decreased vascularity and potential loss of scrotal skin. What was probably not mentioned to you at the time of the injections was that it was a one way street. Once you get that mass of silicone and surrounding scar into the scrotum, you are not going to get it out without creating its own set of potential complications . In short while that theoretically will create more intrascrotal space, it will not improve the success of testicle implant placement or decrease their potential risk of complications. In fact trying to remove this scarred mass probably increases implant-related risks.
2) The real question is then can testicle implants be successfully placed into the scrotal tissues that now exist.That is a question that is hard to answer and would depend in my opinion on how soft or hard the scrotum now feels.
3) But what I am certain of is if testicle implants can be placed into the tissues, careful consideration needs to be given to their size. This is no longer a situation where putting in the maximum size now exists. This is a compromise situation now.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am currently consulting for bimax surgery (le fort I + BSSO with CCW rotation). I have mild OSA so there is some health justification, but if I am being honest my concern is primarily aesthetic and I do not think I would go through the cost and risk if there were an easier/better option. I have been told by some that jaw surgery is the only way to address my retrognathic mandible satisfactorily, and that genioplasty would produce subpar result (the chin would be jutting out, and would mess up my labiomental groove, etc)
I am trying to figure out what other options there might be from a purely cosmetic angle and have heard good things about your clinic in terms of chin augmentation that is more sophisticated than common genioplasty you would get from the local plastic surgeon.
A: I believe what you are asking is whether a sliding bony genioplasty or even a custom chin implant would produce an aesthetic result comparable to that of a BSSO +/- genioplasty. Certainly that is a fair question given the magnitude and process of double jaw surgery. All I can really say just looking at a lateral cephalometric x-ray is that the horizontal projection of the chin needs to be at least 12mms, maybe a bit more. This indicates that a bony genioplasty would be the better procedure as opposed to an implant. But how that would look on you and its effects on the lower lip and labiomental fold requires computer imaging of your facial pictures to determine if you see that change as a desirable aesthetic improvement or that it looks unnatural.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr, Eppley, I’d like to get started on the process of consulting and booking with you. I am very interested in a form of genioplasty (chin shield?) which could improve the chins height, width, and projection. I currently have 2ML of chin filler injected earlier this year.
I am on the fence about lateral commisuroplasty and submentoplasty, and would love to hear your thoughts on how beneficial they would be for me. My mouth is narrow for my face but the risk of scarring scares me, and I believe I genetically have a low hyoid bone and am prone to storing submental fat.
 A: Thank you for your inquiry and sending your pictures. There are numerous bony and implant methods for chin augmentation not all of which can produce identical three dimensional chin augmentation changes. Since you have specifically mentioned all three dimensions (projection, height and width increases), such 3D changes can only be done by an implant, specifically a custom designed implant. But before we get into how your chin augmentation should be done, let’s first begin the discussion about what exact chin shape changes you are seeking. In that regard I have attached some initial computer imaging to begin that discussion. (see attached)
A: Thank you for your inquiry and sending your pictures. There are numerous bony and implant methods for chin augmentation not all of which can produce identical three dimensional chin augmentation changes. Since you have specifically mentioned all three dimensions (projection, height and width increases), such 3D changes can only be done by an implant, specifically a custom designed implant. But before we get into how your chin augmentation should be done, let’s first begin the discussion about what exact chin shape changes you are seeking. In that regard I have attached some initial computer imaging to begin that discussion. (see attached)
As for the ancillary procedures, combining chin augmentation with submental liposuction has obvious benefits and there would be no reason not to do so. You have said all I need to know about the mouth widening procedure…the best way to avoid the risk of adverse scarring is not to do it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am scheduled for Bilateral Anterior and Posterior Temporal Muscle and Bony Temporal Line Reductions. My question is:
“How long would it take after the temporal surgery for all the swelling and wounds to completely heal? I have a hair transplant procedure that I’m going to reschedule to a date after this surgery and I was wondering when’s the earliest date I could postpone it to.”
A: I would at least two months after this surgery to do a hair transplant.
Dr. Barry Eppley
Indianapolis, Indiana