Your Questions
Your Questions
Q: Dr. Eppley, I have a theoretical question about a subcostal rib cage implant for one side of my body. I was born with underdeveloped and thinner ribs on one side of my body (a rare variation of poland syndrome). IT is not from anything, they are actually thinner on my right side as my chest too with even strength on both sides is very unequal in thickness no matter what I do. I could get rib shaving on the other thicker rib cage to even it out, but the problem is my hips are too bulky for that. Because of this underdeveloped rib cage, my right side abs don’t really go out in front of the hip or level making the hip look really bad and buldgy and my abs aren’t at the same level which looks really off. ISS there any implant (Im assuming a rib one) that could be made that would push those right rectus abdominal muscles a bit further out to match the other side? Also this unevenness in my rib cage is also present in my chest thickness (Going to have an implant in my right chest to help feel straighter because I always feel crooked) but could the same thing be done with the rib cage below the chest? I can’t find a good picture that depicts the uneven level of the abs but it is very apparent visually.
A: Thank you for your inquiry and detailing your body contouring needs. What you have described is very possible because the subcostal rib cage is largely covered by the upper portion of the rectus abdomins muscle. This provides the opportunity to place an implant on top of the ribs but under the muscle which would do, just as you have described, push out the right rectus abdominus muscle. Not only would this create that effect but also places the implant in the most favorable location. (submuscular location)
Whether the same concept applies to higher up on the chest requires a better understanding of the actual chest wall deformity as well as where that is location compared to the pectoralis major muscle attachments.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m very interested in hip implants. Is after hip implants is a bbl possible. But I want also transfer the bbl fat in my hips. Is this possible too? Or should I make first the bbl? Is the doctor also doing bbl? If yes, is it possible make a bbl when I have butt implants? Or did the doctor need them take out?
A: In answer to your hip and buttock implant questions:
1) A good candidate for successful hip implants is based on two criteria: 1) adequate subcutaneous tissue thickness over the hip area (which you have) and 2) moderate but not extreme hip augmentation goals. (which in you I do not yet know)
2) Fat transfer to the hips should always be done first, if one has adequate fat stores to do so, before undergoing hip implants.
3) Fat transfer (aka BBL) can be done with intramusculr buttock implants and is known as composite buttock augmentation surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Can you reduce a high spot the skull to make it level with rest?
A: That would depend on the thickness of the bone and how much it will permit the high spot to be lowered. How they applies to you requires a picture of the high spot at a minimum and ideally a 2D skull CT scan to measure the thickness of the bone at the high spot.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had coup de Sabre since I have been in 5th grade (10 years old ) mainly affecting my forehead and part of my scalp. I have been looking for doctors that are willing to do cosmetic surgery on my forehead to bring it back to its normal state but none have been willing. I have had consultations about this disease but never had answers. I came across this article of your procedure on a patient with my same condition and would love to have this procedure done to make me feel better and more confident with my look. Coup de Sabre has affected me in many ways. I hope to speak soon. Thank you for your time.
A: Thank you for your inquiry and sending your picture. I have treated numerous cases of linear craniofacial scleroderma, most of which have affected the forehead and scalp along the distribution of the supraorbital nerve. In treating the forehead contour deformity the brow and forehead bone is deficient as well as the overlying skin is thin. I have treated it with both bone cements and fat grafting and each has their own advantages and disadvantages. In the end the problem is both a combination of bone and soft tissues so ideally both are eventually needed for optimal results.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I read your website about waist narrowing/ribs removal surgery, and would like some more info. I have had a lot of surgeries so far, including 3 breast implant surgeries to take me to my current size of 2200cc. Also have butt implants and bbl, and want the extreme hourglass figure. I am totally into the fake plastic barbie look, and want to go all the way with this.
I’m quite small build, and the breasts is taking up much of my ribcage. Is having xl breast implants something that influences ribs removal surgery? I am going to get another redo on the breasts later this year to go bigger.
Attaching some pics of myself. Do you think I’m a good candidate for ribs removal surgery?
A: You are a good candidate for rib removal waistline narrowing surgery for two reasons:
1) In the spirit of making the maximal effort for the extreme hourglass look, you have addressed the breasts and buttocks above and below the waistline but have not yet done the waistline itself. So the third member of what contributes to the hourglass shape remains unchanged.
2) Women with the thinnest builds actually get the best waistline narrowing results because the fixed anatomy of the ribs is making the greatest contribution to its shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, To indicate the type of cheek changes I am looking to make I can only really represent those changes using photos other people that have the features. Essentially, I want to be able to have an ogee curve with the high angular cheekbone look directly underneath the eye which is associated more to a masculine 3/4 profile as well as hollow cheeks that contour as a result? I’m unsure about my facial structure generally and with where it currently stands, are my cheekbones already high but projecting more laterally? is it just that they are not anterior projecting enough therefore cannot replicate the look I’m referring to? What would you advise I do next?
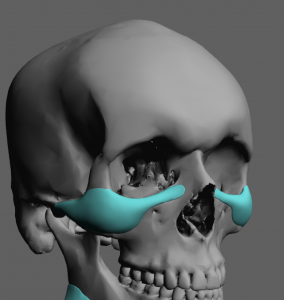
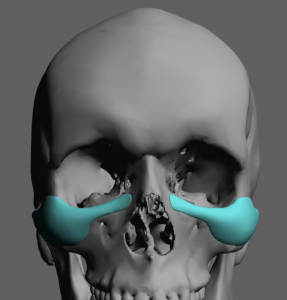 A: You are fundamentally talking about some version of the high cheekbone implant which is designed to create that type of ogee curve change. (see attached) Whether that would have that effect in your face depends on what your face looks like which remains unknown to me at this point.
A: You are fundamentally talking about some version of the high cheekbone implant which is designed to create that type of ogee curve change. (see attached) Whether that would have that effect in your face depends on what your face looks like which remains unknown to me at this point.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently considering forehead augmentation surgery to make my forehead less sloped, more symmetrical on each side and more prominent at the front. I wanted to ask whether adding additional PEEK material or bone cement will automatically change the top of my head shape slightly, as this is connected to my forehead. I also ask this because I had previous surgery where the forehead bone was shaved down very thinly and in the process my frontal skull/head connected to this forehead area also became very flat at the top and front. Please note that the top of my head was not touched in the previous surgery, only the forehead bone was shaved down. I noticed that in the picture below, the top of the patients head also changed shape slightly and appears higher and less flat (like the forehead) after forehead augmentation surgery. Could you please advise me on the cost of the same procedure or by using peek implants instead?
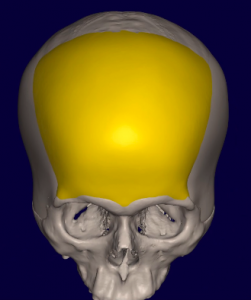
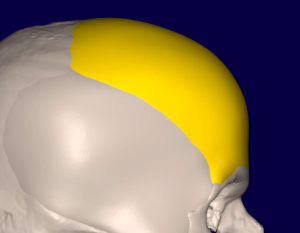 A: Like all forehead augmentations, it can not just stop at the top of the forehead unless the forehead augmentation is but a millimeter or two. As the slope of the forehead becomes less the implant design must extend further back onto the top of the skull and over the sides of the bony temporal line onto the temporal fascia to blend into the rest of the skull. (see attached)
A: Like all forehead augmentations, it can not just stop at the top of the forehead unless the forehead augmentation is but a millimeter or two. As the slope of the forehead becomes less the implant design must extend further back onto the top of the skull and over the sides of the bony temporal line onto the temporal fascia to blend into the rest of the skull. (see attached)
Because of the need for these extensions and that they be smooth and very feathered, the use of bone cements has largely been abandoned. This requires a computer designed implant. Unless one wants a full coronal scalp incision to place the implant this is also why PEEK and any other completely inflexible materials are also not desired by most patients today. Solid silicone skull implants offer the far superior method for any form of aesthetic skull augmentation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have had a full-chin-wing procedure about 1.5 years ago. The chin was forwarded by 4mm, giving me a harmonious side-view. However, the front view is unpleasant, since the jaw angles were blunted, leaving me with a U-shaped jaw line.
I am very interested in reversing this procedure. I have heard from several sources that it should be possible to reverse the changes made, by doing a revision chin-wing. I would like to hear your opinion about this.
As far as I have understood, the implanted hip-graft, which will be full fused with the bone by now, shall be removed. Thus making it possible to establish the old jaw position.
Is it possible to precisely remove the fully fused hip-graft, in order to reverse the changes caused by the first procedure.
I would very much appreciate your opinion on this matter.
A: Like all chin wing procedures it is a chin-anterior jawline procedure which has no effect on the jaw angle area. It can not improve the jaw angle length or width. Often it can even make the jaw angle look worse by comparison.
I see no reason that the chin wing osteotomy could not be recut and returned to its original position. Where the hip graft is located along the jawline is unknown to me but it has undoubtably healed and integrated into the surrounding bone at this point. Whether it can or needs to be removed in this chin wing reversal I could not say based on a description alone. You would need a 3D CT scan of your lower jaw anyway prior to the procedure and the location of the hip graft and its fate would then be able to be determined.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in surgery to help fix my facial / cranial appearance and to help me feel like i can easily have a good neck posture. I have a weak chin, jaw, and cheek bones. My orthodontist agreed with me and has x-rays but said she couldn’t do anything to help. In addition i feel like my head is misbalanced in that most of my weight is the back. I did not have the benefit of positive horizontal facial cranial growth forward. For years i’ve felt awkward trying to have a natural neck position. When I try to have a natural neck position most of my face looks squished and most of my head is balanced in the back making it difficult to keep this position. In addition to trying to keep my natural neck position it is hard to talk. Maybe i’m over correcting my posture at that point but it’s hard to know without a medical profession correcting me with what is actually natural. Over the years my neck posture has gotten worse and have neck pain because i’m trying to look “normal” without my face looking squished and my natural propensity to keep my head slightly forward so i can talk correctly. Keeping my head forward from a natural neck position isn’t very comfortable on the neck.
The follow pictures will show my side profile and front profile. I would like the doctor’s opinion on my comments and my pictures. Is there anything that could be done? At the very least I would like to improve my neck posture and have a “normal” side profile.
A: Thank you for your inquiry and sending your pictures. While there are procedures to help with your jaw deficiency (custom jawline implant) and protrusion of the back of your head (occipital skull reduction) which will have aesthetic benefits (see attached imaging) I would not expect that to change how you hold your head. (neck posture) Neck posture is a learned behavior. It is possible that you hold your head that way because of your short chin/jawline and these aesthetic improvement may help, but any improvement in your neck posture should be perceived as an unexpected bonus and not an expected outcome from these surgeries.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was curious would a being on bone canthoplasty increase pfl? Also do you think raising my cabthal tilt would benefit me? I had a canthoplasty 3ish years ago. I’m not completely happy with it. I think my right eye is definitely better than my left, ( but I think both of them could benefit from another one.
A: While I don’t know the lateral canthoplasty technique that was done and what you looked like before it I can not say with certainty whether more tis o be gained by a secondary lateral canthoplasty. But in just looking at your lower lids it appears that it may be likely with the caveat that combining it with spacer grafts is the more assured approach. (the concept being that if one wants a different outcome than the first time plan B should not be identical to plan A)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, as I am getting older my hair is thinning and my hairline is receding, and I am now noticing a strange and seemingly out of place shape on my head. It resembles the shape of a half egg and it is awkwardly planted in the center, just above my forehead. When I was younger, my mother may have noticed it, but she would never talk to me about it, so I presume its always been there. I’m hoping theres an answer to this, I feel self conscious over it.
Hello, I have a noticeable ‘bump’ in the center-front portion of my head. If you look at me from a profile angle, you may not notice it. If I look forward and straight ahead, it also might not be noticeable. But if I look up, then I have a bump the shape of a half-egg on tope of my head. I’m getting older and I no longer have as much hair as when I was young. It makes me self conscious and I’d like to look into possible solutions.
A: Thank you for your inquiry and sending your pictures. You are undoubtably referring to the raised midline prominence at the anterior end of the sagittal suture line. (which is also the original location of the anterior fontanelle) This raised bony prominence is probably a thickened area of bone which can be reduced by burring. BUT one should first check a CT scan to be sure that this is really a thickened area of bone rather than a thin area of bone with the underlying brain protruding into it. (unlikely but the time to make that discovery is before surgery not during it)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Been looking around for the time of healing for the procedure of occipital knob reduction.
A: The time of healing after occipital knob skull reduction surgery depends on how you choose to define ‘healing’. I suspect you actually mean recovery as that is more relevant. True 100% healing of the tissues is 2 to 3 months. Recovery from the surgery is very different at 7 to 10 days maximum…if that.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in Iliac crest implants and rib removal. Is it possible to do both of these procedures in the US?
A: Both rib removal waistline narrowing and iliac crest implant surgery can be done at the same time. Here in the U.S., unlike Korea where the original titanium iliac crest implants were developed and remain unapproved by the FDA for U.S. use, ultrahard solid silicone iliac crest implants have to be used.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m considering undergoing V-line surgery but I’m afraid if I do I’ll get an overly oval/egg shaped face with a jaw that is too narrow. Is it possible to get V-line surgery just to change the height of the ramus and with some overall narrowing but not too much?
In particular, I dislike how low my jaw/gonial angles are in relation to my mouth; I would like my jaw to have more of a V-shape but with higher jaw angles, like in the picture I attached. I have also attached my own photo.
A: You are wise to be concerned about V line surgery for your facial goals for the following reasons:
1) The way V line surgery has to be done due to the intraoral approach and the use of 90 degree saw angle is a major vertical jaw angle reduction. It is technically impossible to just due a ‘little’ vertical jaw angle reduction and/or keep some jaw angle shape. This is a relatively drastic jaw reduction procedure when it comes to most Caucasians faces and lower jaw shapes. So the concept of ‘not too much’ jaw reduction is usually not a realistic one.
2) Postoperative regret amongst Caucasian V line surgery patients is much higher than in Asian V line surgery patients.
3) The ideal image you have shown compared to your face is probably not a realistic change. Plus your face picture is taken straight one while the ideal one is tilted down…that little change makes a big difference in its appearance.
4) Patients often overlook the fact that the face is a 3D structure. How it may be seen in one view (in this case the front view) may be very different from other angles. (side or oblique views) So even if that type of change was possible you may very well dislike how it looks in other views…. a common postoperative ‘finding’ by some patients.
5) You may find that reduction of the width of your jaw angles only may achieve the lower facial shape change you desire without the negative aesthetic effects of traditional V line surgery. This is often effective in patients that don’t want too much of a change to the jaw angle region of their lower face.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 1. How wide can a skull implant possibly ? Considering one does a scalp extender and does anything necessary to achieve that. I’ve seen it be 7mm at the widest point and then another 1cm or more if im not mistaken. How much further can it exceed?
2. I’ve read that you never go past 350cc is it possible to exceed this as well or would this volume be great enough to make a small skull into a large one?
3. Have there been any time where you’ve seen a person will a disproportionate small skull transform into someone with a large skull with the changes being immense?
4. People who have small heads also have even smaller foreheads. When making skull implants are you able make the forehead the same length as the back after you’ve already widened it from the back.
Thank you for your time.
A: In answer to your skull implant questions:
1) As a general rule there would rarely be a need to ever go over a 7mm head width increase. It is important to remember that this is bilateral so the effect is a 1.5 cm head width increase. Also almost every skull implant patient way over estimates what their implant dimensions should be. Patients focus on linear measurements which is not reflective on what volume does over a large convex surface.
2) A 350cc implant volume on the head is substantial. Whatever it achieves in any patient would be viewed as a substantial change.
3) The interpretation of any aesthetic change is highly individualized. So what the term ‘immense’ means can only be determined by each patient.
4) Your interpretation that the augmentation of any skull surface must be done with an appreciation of how it looks in relation to the rest of the skull is an important one. As skull implants become bigger in size their surface area coverage must become similarly so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to do anterior, posterior, lateral, and above skull implants together, but not on the same day?
A: That is technically possible but would not usually be a good aesthetic choice. The skull is a large connected set of convex surfaces so augmenting all five skull surfaces independently would not make for a smooth external appearance unless each implant was very small. (thin)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello. I want to reshape my head with bone cement. The first image is before and the 2nd is what I would like (used photoshop). Is this possible?
A: You are not going to get that skull augmentation result (or even close) with bone cements for the following reasons:
1) The most common bone cement (PMMA) used in the skull is a plastic material and does not turn into bone. It is in fact a plastic implant so don’t let the name mislead you. It is the same material that is used to cement in orthopedic joint replacements. When used in the skull the manufacturer simply puts it in a different package and calls it Cranioplast.
2) The other type of bone cement (HA or hydroxyapatite) is a synthetic phosphate (ceramic) that does not turn into bone either. It may be a distant cousin to bone but is still an implant. It was developed for the use in cranial defects (inlay) not onlay (on top of the bone) augmentation. While it can be used for small skull augmentations, it is too brittle to do large ones. Of equal importance its cost precludes its use for most aesthetic patients. At over $100 per gram the cost of the material alone (large skull augmentations are in the range of 150 to 200 grams or greater) would be in the range of $20,000.
3) Even if #1 and #2 were not issues with bone cements for skull augmentation, they require wide open exposure for placement which means a full coronal (ear to ear) scalp incision is needed.
4) Bone cements can only be placed on bone and can not be applied over soft tissues areas. (side of the head) The larger a skull augmentation is (more projection) the more its base needs to be wider and cover more surface area so the result does not look like an unnatural bump on the head. This means the augmentation has to wrap around onto the sides of the head which are soft tissue covered (temporalis muscle and fascia) onto which bone cements can not be applied. (will not stick to it)
In summary bone cements have a very limited role in aesthetic skull augmentations and only have merit in small skull augmentations that are usually in the 50 to 60 gram volume….a result that is a far cry from the one shown in your own skull augmentation imaging.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, At the moment I am undecided as to whether I want bone burring to be done due to the bi-coronal incision (incision that travels over the scalp) so I just want you to assist me in weighing up the risk to benefits by answering some enquiries. I also say this based off a recent Instagram post of yours demonstrating this surgery which is shown in the image attached image. It is to my satisfaction that these incisions in the image look quite simple and much less invasive compared to the approach we have planned for myself hence why I have these enquiries:
-Based off my CT scan, if you were to bone bur the temporal line, what is the most in millimetres that you could reduce and would this reduction be noticeable?
-Would I still achieve forehead narrowing if I just had anterior & posterior temporalis muscle reduction without any bone burring?
-Have you ever had patients encounter shock loss with hair from this large incision ?
-If the large scalp incision was done, how long would it take for stitches to close up and heal?
-Is there an alternative incision in achieving bone burring?
Your answers to these enquiries would influence me in deciding if an incision that large is worthwhile doing as I’m starting to feel that I’ll be the most comfortable with the approach shown in the image below.
A: You can’t do the type of bony temporal line and anterior temporal muscle reduction that you seek through the anterior temporal incision shown in that picture. That does not apply to your case.
Bony temporal line reduction is always at least 5mms, which when done bilaterally (or even unilaterally) makes a visible external difference. Your case is no different in that regard.
Temporal muscle reduction of any type will not change forehead width. Foreheasd width reduction is controlled by the bony temporal line.
The only hair shock loss I have ever seen in larger scalp incisions is when it is used for large skull implants or tissue expanders (which is very uncommon)….not with any form of skull reduction which is what I would expect with a total lack of tension on the incisional closure.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, i have consulted with a surgeon about the procedure modified lefort 3. My question is why is the implant route the way to go instead of surgery?
A: The midface implant route is the superior aesthetic approach to midface augmentation IF there is no compelling need to change the occlusion. (one’s bite) It is superior to a LeFort IIII in an adult because:
1) Every midface dimension/thickness can be precisely controlled by the preoperative design.
2) It provides a complete midface augmentation effect particularly in and around the orbit rim and malar region.
3) It provides an assured smooth contour.
4) It is less invasive with a quicker recovery.
5) It is reversible or capable of being modified (addition/reduction) should one want to fine tine the result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding facial outline and skull shape. I have looked through your question archives but couldn’t find anything on the exact topic. Is it possible to change the facial outline of your face to make it less round and more straight. I am including a picture as an example. My facial outline is round. The model has a straight facial outline which is well defined. I understand that buccal fat can be removed for less round face but I am asking about the outline of the face and not the cheeks. Thank you
A: Without having a reference point (your picture) I can not say whether your face and what could be done to change to make it more straight is possible.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I believe my jaw is not symmetrical and feel one side is longer.. if I sent a variety of photos that it is very visible could you possibly tel if it can be solved/ corrected my by just a custom jawline implant or chin implant or if I would have to go down the path of jaw surgery and jaw reconstruction!
A: I would be happy to review your pictures of your jaw asymmetry but, even without pictures, there is certain known principles treating it based on my experience:
1) A 3D CT scan is the definitive method to fully understand the exact bony anatomy of the jaw asymmetry.
2) A chin implant can never adequately treat jaw asymmetry and often when done alone makes it more apparent as the asymmetry increases as it moves from the chin back to the jaw angles.
3) In some cases a unilateral custom jaw implant on one side may correct the asymmetry if it has a modest amount of bony asymmetry.
4) A total wrap around jaw implant is usually the definitive treatment for jaw asymmetry as the discrepancy between the two sides usually merits it and many men decide to provide some overall lower facia enhancement as well.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to ask for your thoughts on what you believe would be the best treatment option for me. I have always had a very ‘flat’ face with lack of forward projection. I am 26 now and previously had braces aged 16 to correct a slight crossbite, and also my upper and lower teeth ‘met’ instead of the upper coming over the lower. I now notice mid-face concavity, deep nasolabial lines and I feel my chin juts too far forward. my cheekbones are flat and there is no projection at all in the apple cheek region. There is also a lack of bone support in the infra-orbital area which I feel pulls my eyes down at the outer corners/ gives me a negative tilt. After much reading online I think I have a recessed upper jaw but I don’t feel its significant enough to undergo orthognathic surgery as I imagine that’s quite a traumatic procedure! I was thinking facial implants may be a good option, but I am unsure which type, or where would be most effective. Ideally id love to achieve a more sculpted, ‘forward-grown’ face, with more defined cheek ‘bones’, forward projection, more apex in the nasolabial area and get rid of the bottom jaw ‘jutting’ out appearance. A stronger overall facial structure with more light and shade/ definition. I will add some pics for your reference!
I greatly appreciate you taking the time to read my message and I look forward to hearing back from you at your earliest convenience.
 A: With an overall midfacial hypoplasia and I assume a reasonable occlusion (bite) the most effective treatment to ‘pull’ your midface forward is a custom midface implant. (see attached) Augmenting the infraorbital rim and downward across the face of the maxilla, it will add total midface fullness without adding any facial width. The custom midface mask implant has the advantage of being a single piece. There are standard implant options to consider (infraorbital, cheek and premaxillary-paranasal implants) which can be put together to try and create a similar effect but i would only consider placing unconnected implants in the midface only of that were the patient’s preference.
A: With an overall midfacial hypoplasia and I assume a reasonable occlusion (bite) the most effective treatment to ‘pull’ your midface forward is a custom midface implant. (see attached) Augmenting the infraorbital rim and downward across the face of the maxilla, it will add total midface fullness without adding any facial width. The custom midface mask implant has the advantage of being a single piece. There are standard implant options to consider (infraorbital, cheek and premaxillary-paranasal implants) which can be put together to try and create a similar effect but i would only consider placing unconnected implants in the midface only of that were the patient’s preference.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a dent in my nose and I find it extremely hard to breathe out of my nose over the years I’ve tried multiple different nasal sprays, home remedies, I’m sure I’ve tried every single suggestion on the internet not only is it extremely difficult for me to breathe I absolutely hate the dent in my nose it’s my biggest insecurity.
A: By your own description you probably have an internal nasal deformity (septal deviation, turbinate hypertrophy or both) which is the primary source of your airway obstruction. The dent in your nose that you refer to is what is known as a bifid nose, meaning the lower alar cartilages are wide and spread far apart creating a valley or groove down through the tip of the nose. Both can be corrected by open rhinoplasty surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I currently have large posterior PEEK jaw angle implants (~12mm width; no vertical augmentation). My presentation is complicated by significant bilateral masseter dehiscence, as I have history of prior jaw surgeries. The appearance is the classic skeletonized angles + the muscle bulge superiorly.
I have read your various posts on masseter muscle reattachment via external approach both on your blog and on forums. I discussed this with my prior surgeon. However, he/she does not think it’s a good idea to do an external surgical reattachment of the muscle to the inferior border of the implants out of fear this may cause masseter tearing, as, given my history of surgeries, there is likely fibrosis within the muscles. In addition, my implants are large.
Instead, the surgeon has recommended 3-4 Botox regimens over the course of a couple years, which he/she said would help the muscle “fall back down” over the inferior border. He/she said repeated treatments would eventually cause some degree of permanent atrophy and could help eliminate the appearance of the superior bulge.
I don’t like the idea of using Botox. In addition, I prefer more permanent solutions.
My questions are:
1) Is the risk of masseter tearing a reasonable concern when considering masseter reattachment for the treatment of dehiscence.
2) Would you ever recommend Botox as an effective non-surgical treatment for masseter dehiscence, or is this truthfully just a fairly ineffective alternative.
A: In answer to your masseteric muscle dehiscence issues:
1) Botox injections are a reasonable treatment option with the understanding of the following:
a) Their effects are usually temporary and have to be repeated.
b) Even with repeated injections any sustained permanent muscle reduction effect may or may not occur. (I have never seen it happen yet)
c) The appearance of the muscle bulge will definitely become less but the muscle will not fall back down. This is biologically impossible as it is a contracted muscle mass now. It will not unfortunately just ‘relax’ and go back into place. This is known as magical thinking.
d) At best Botox will produce a lessening of the muscle dehiscence appearance but it will not make it go away completely.
2) The risk of masseter muscle repositioning is not whether the muscle will tear but whether it is so fibrotic that it simply won’t move much. (unsuccessful repositioning) The other thing you have to consider is how to fix it the muscle to the PEEK material if you are fortunate enough that it is capable of being mobilized.
3) Any effort at masseteric muscle repositioning must be preceded by Botox injections to get the muscle to relax/soften a bit. One or two rounds of Botox, preferably two, before such surgery improves the chances of success.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My little boy is soon to be 6 years old. He has a wide head with flattening mainly to one side and his ear is slightly pushed forward on that side.
I would like to try and get this sorted for him before at this age. Is this something you can help him with?
I think you can use a skull cement that can be used at his age? Is this very costly? And is it effective? Does it leave much of a scar? How long does it take?
We are based in the uk but I don’t think this can be done in the uk?
I am really keen to sort and how do we progress with this?
A: When it comes to treating occipital plagiocephaly in children the only good option, in my opinion, is hydroxyapatite cement. While such HA cements don’t really turn into bone, the body does view them as more ‘natural’ and develops osseous integration with the surface of the skull. While such HA bone cements are the ideal material they are not perfect and have several notable downsides which include the following:
1) Placement of them requires direct visual access to properly place and shape the cement. This means that a longer scalp incision is needed to do so.
2) Any bone cements have to be placed exclusively on the bone or otherwise they will fracture. Since plagiocephaly skull deformities wraparound the side of the head into the posterior temporal muscle region, such corrections are imcomplete.
3) HA cements in the U.S. are very expensive compared PMMA acrylic bone cements. But PMMA is a material that should not be used in children due to the growing skull.
For the reasons so stated above I advice parents to wait until the teenage years when a more effective method in treating plagiocephaly exists (custom skull implant) and the use of these other more effective materials are placed in a skull that has undergone much of its development.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I would like to ask about the customized skull, how hard is it and is it safe and almost as hard as the original bone?
A: A custom skull implant will feel just like bone and when implanted you can not tell the difference between it and your natural skull….even though outside the skull it has some flexibility and is not as rigid/stiff as bone. It is a common misconception that an onlay (on top of bone) skull implant should be as hard as bone…that is wrong. It is an inlay skull implant replacement for full thickness defects which should have a stout rigidity to it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, in terms of the occipital procedure, what kind of swelling can I expect and will any hair be shaved to make the incision? Or in other words, will I be able to go back to work pretty soon afterward without worry about the scar being seen as it’s healing and any swelling being noticeable?
A: In answer to your occipital skull reduction questions:
1) No hair is shaved for the procedure.
2) Most of the swelling that occurs is on the back of the head and does not affect the face. So it is really not that noticeable to others. So you should be able to go back to work fairly quickly.
As for the forehead one treatment option that we did not discuss was fat injections, a minimally invasive procedure with virtually no recovery. While it is not what I would consider for medium or larger types of skull augmentation but for small contour concerns it is an option.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m curious are there any surgeries to make the eyes look further apart? I know an orbital box osteotomy actually moves the eyes further apart but that’s a obviously a very invasive surgery for a couple of mms.
A: Whether it is 2mm or 10mms the only way to physically move the eyes further apart is with the orbital box osteotomies. Admittedly the lesser the amount of separation needed the more the orbital box osteotomies is a solution that is much bigger than the problem merits.
Dr. Barry Eppley
Indianapolis, Indianapolis
Q: Dr. Eppley, Hey I’m a transgender female patient who is interested in getting hip implants cause I have hip dips and they make me feel like I look boyish.
A: Of all body contouring procedures, hip implants have the highest rate of postoperative problems. I have learned to choose patients carefully for this procedure to lower these complications risks. My preoperative assessment includes pictures of the patient’s hip areas with imaging predictions of what I consider realistic outcomes. The patient’s soft tissue thickness is also a key consideration. Thin tissue patients with little subcutaneous fat have a high risk of implant show/edging.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had an endoscopic brow lift 3 years ago and I am left with 4 vertical lumps on my forehead (pictures). The surgeon who did the brow lift believes it is scar tissue.
Do you think you could treat those scars by any means ? Would it require surgery or maybe just steroid injection ?
Thank you
A: This is a most unusual sequelae from an endoscopic browllift that I have never seen or heard of before. While you can certainly try steroid injections I would not expect that to provide any improvement. I don’t think this is scar tissue nor could I biologically explain why such scar tissue would occur along these very specific vertical ‘lines’ since in an endoscopic brow lift there are no periosteal/galeal tissue releases done along these lines. There are only vertically ‘pull points’ located at the scalp incision locations. My speculation would be that this is more likely related to the vertical pull of the browlift which has created tension lines in the forehead. I don’t think it is a coincidence that the tissue lumps are vertical in orientation and that the browlift is based on a vertical tissue pull.
If that is a correct theory then the only solution may be a horizontal release of the galea of the forehead as is more commonly done in open forehead procedures. What is clear that at 3 years postop this is not an issue that time and tissue relaxation will solve.
But I make these comments based on only seeing two pictures and having no specific knowledge of the endoscopic browlift technique
Dr. Barry Eppley
Indianapolis, Indiana