Your Questions
Your Questions
Q: Dr. Eppley, I am writing this email with regards to a Jaw reduction surgery I had 8 months ago. I initially went with regards to minimal asymmetry in my chin. I asked about a genioplasty procedure to address this.
The maxillofacial surgeon proceeded to say that my chin was very broad and that I had a square face shape and this was a bony deformity. My 3D CT face scan was compared to images on Google of a ‘female skeleton’ image and a ‘male skeleton’ image. The surgeon then went on to say that my face resembled the male skeleton and that my face was masculine. I was very self-conscious and shocked to hear this. I was then told the only treatment option to address this was a ‘facial contouring surgery’. I was told that they were offering the newest and latest surgery technique. I was also told that it would be a modest surgery and the only side effect from surgery would be lip swelling. I was told that I would see a better version of myself and the results would be minimal.
I was misled and deceived about the nature of the surgery. The finalized ‘bony cuts’ were never shown to me and I was not even made aware of how much bone in mm would be reduced. I did not anticipate a dramatic reduction of this nature and that I did not want a reduction along my entire mandible.
Unfortunately, the surgery has resulted in an overcorrection. The left side of my jaw angle has been removed (reduced by 17mm) and the right side jaw angle was not removed. I have more asymmetry in my jaw which looks very unpleasant (left side being more deficient). The jawbone surrounding my chin has been chiselled off leaving me with a much narrower and distorted chin. I have muscle/tissue balling and bulging in my chin and I am also unable to move my lower lip. I have also developed a lot of scar tissue.
I have been devastated and aggrieved by the jaw surgery for the past 8 months, which significantly added to my depression. I have had no support from the surgeon who has conducted this procedure on me. I have arched my post-surgery CBCT face scan here and I also have reports (measurements in mm of both left and right side of my mandible) and I also have 3D models of my Pre-Surgery and Post Surgery mandible.
I am looking for a correction surgery to recover my original jawline and reconstruct my mandible skeleton.
Hoping for your guidance and kind perusal on this matter. Many thanks.
A: Like some jaw reduction surgery patients the outcome is unsatisfactory due to either over correction and/or asymmetry. If this was an effort at v line surgery or even jaw angle reduction, the after surgery 3D CT scan speaks for itself. Fortunately the right jaw angle remains unchanged so the issue is really the left side. A custom left jaw angle implant would suffice for returning the bone as close back to preop as possible.
I can not comment on the chin as there are no front views provided of either before or after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a young male with mild hypertelorism and this given me cosmetic pain for a long time.
I heard that patients with mild hypertelorism undergo orbital wall osteotomy, not orbital box osteotomy. Box osteotomy is burdensome. The range I want to correct is about 4mm. And I don’t have the Mongolian folds that are characteristic of Asians. I don’t need soft tissue surgery.
I want to correct it with an extracranial approach, but I don’t have much information.I heard that you wrote a thesis on this.
A: When you refer to an extracranial approach to mild hypertelorism correction you could be talking about a variety of procedures. One approach is medial wall infracture with lateral orbital wall implant to push the eye inward a few millimeters. For small amounts of hypertelorism improvement this can certainly be a less invasive way to achieve it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like my forehead slope reduced, as much as possible. I figured it would involve a bit of brow bow reduction, forehead implant and hairline advancement surgery.
A: By your description maximizing the forehead slope reduction would be done by inferior brow bone reduction and forehead implant augmentation. Frontal hairline advancement is more about decreasing the visible length of the forehead not necessarily about changing its slope. But when the other two are done bringing the hairline forward does eliminate the part of the forehead that starts to slope backward no matter how much the forehead is augmented.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, A person who has already had a canthoplasty (almond eyes surgery) or an infraorbital implant can have a zygomatic arch implant placed without damaging the prior canthoplasty or orbital implant?
A: The best method for placement of a zygomatic arch implant is through the lower eyelid where direct linear access to the arch can be done. This is the most assured method of getting them into ideal position and with good symmetry between the two sides. Would that disrupt the prior work…probably not. But if those areas can be avoided that is the 100% assured way that it would not. That leaves the intraoral route to do so…the most difficult way to place any implant design that has a long zygomatic arch component.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in a scrotum augmentation with XL implants of approx. 7cm. Do you have testicular implants that are 6 or better 7 cm in size or do they have to be specially made? Is it even possible to insert 7 cm implants into a normal scrotum or does a 6 cm implant have to be inserted beforehand?
Kind regards
A: Any ultrasoft solid silicone testicle implant larger than 5.0cms has to be custom made. We have all such computer designs from 5.5cm to 7.5cms already on file so they can be quickly manufactured when needed. I think that a scrotum with normal sizes testicles is NOT going ti be able to accommodate two 7cms testicles immediately….that is simply too much volume for even the very stretchable scrotal skin to be able to safely do. Two 6.0cms implants would be more reasonable to do.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, my head is extremely extremely small and flat. Basically like microcephaly making me look like a monkey when I expose it. Can anything be done to round it out? Also, will this procedure affect hair growth?
A: Skull augmentation with custom made implants for exactly your concerns (small head) are routinuely done. The key question is whether this would need to be a one vs two stage skull augmentation procedure based on how much skull augmentation you need and the ability of the scalp to stretch to accommodate it. How this applies to you is not yet known. Such skull augmentations do not affect the ability of the hair to grow after surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Quick question can a slanted forehead be corrected? There’s a really steam slope on my forehead more noticeable on the profile.
 A: An excessively sloped forehead is a very common indication for forehead augmentation surgery. This is best done by a custom made forehead implant where the degree of slope correction can be preoperatively selected along with important design issues of how far back onto the top of the head it needs to go s well as how to blend into the sides of the forehead around or across the bony temporal line.
A: An excessively sloped forehead is a very common indication for forehead augmentation surgery. This is best done by a custom made forehead implant where the degree of slope correction can be preoperatively selected along with important design issues of how far back onto the top of the head it needs to go s well as how to blend into the sides of the forehead around or across the bony temporal line.
Dr. Barry Eppley
Indianapolis, Indiana
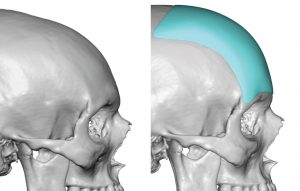
Q: Dr. Eppley, how long does temporal reduction surgery usually takes? And is it done with a scalpel or shaver? I´m curious because of the incision size you know, one thing is the head narrowing but on the other hand its scar after.
And is it only a partial resection of temporalis muscle? Isn’t it necessary – to smooth out with bone cement in case that hollowness might occur?
And if I am right – does the partial temporalis resection look like this?
A: In answer to your temporal reduction questions:
1) The usual surgical time is 90 minutes.
2) Temporal muscle removal is done by a combination of elevators and electrocautery.
3) The incision is limited to the postauricular crease on the back of the ear.
4) Postoperative hollowness has not been a problem due to the eventual atrophy of the cur edges of the remaining muscle left behind.
5) A more accurate reflection of the cut line and the amount of muscle removed can be seen in the attached diagram.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have an inquiry about custom vertical jaw lengthening implants. I have downward swung jaws that make my lower third somewhat long, my gonial angle very high, a short ramus, and very steep jaw (40 degrees). As far as the implants on the jaw go I have 2 questions.
1. Can these implants be created with minimal width expansion? I am not too worried about my jaw width, I don’t need or desire a jaw as wide as my zygos.
2. This is my largest worry: Will the distance the jaw/gonion is lowered translate to the most outward point on my jaw from the front lowering the same amount? I worry that lowering my gonions 1 – 1.5cm will cause my lower face to look blocky and bloated from the front since my somewhat long chin will still exist but now my jaw angles will be below my mouth. Is there any implant design method that can lengthen my ramus but not severely change jaw angle placement?
I am really considering this procedure along with sliding genioplasty in the next year but this second point of contention has me extremely worried.
Thanks.
A: Because they are custom jawline implants they can be made however one deems appropriate. The usual minimal width of material is 3mms. As a general rule few patients with high jaw angles need or are advised to go 10 to 15mms on the vertical jaw angle drop for the very reason you describe as well as the high risk of masseteric muscle dehiscence.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to inquire about the Occipital Bun reduction surgery. What is the cost, recovery time, and potential scarring after the procedure. I have no hair and wear my hair bald so the scarring would be visible and wanted to know how prominent the scar would be. I have attached some photos.
A: I would advise he go to www.exploreplasticsurgery.com and search under Occipital Knob Skull Reduction and look at the many cases done so he can appreciate the small incision used and the resultant minimal scarring from the procedure. There is a very minimal recovery time and I am not so sure I would even call it much of a recovery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I have been looking at some your posts and although you don’t think temporal bone reduction is necessary and muscle reduction is the way to go for a more effective result I just wanted to ask how much of the temporal bone are you able to reduce.
A: The key question is whether the scar up the side of the head is worth it for the additional 2mms or 3mms of temporal bone removal that can be achieved. You can’t do bone removal from the incision behind the ear. In essence for the minor amount of extra temporal width that can be achieved by bone removal the visible scar to so is usually not an acceptable tradeoff. In addition to date no patient who has had muscle removed has ever said they needed additional width reduction afterwards.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been researching possible issues related to my 12th rib. I have both pelvic and rib pain over the last 3 years. Is my12th rib on the right unusually long? I can easily feel it when palpitating the area. I have been struggling to find a diagnosis or treatment plan.
Thank you for any information you can provide. I appreciate your time so much!
A: It is clear from your 3D CT scan the right 12th rib is longer than the left. Most 12th ribs are very short, the shortest of all 12 ribs, so your right 12th rib is longer than normal. Most of the time they are not palpable from the outside. If you have rib/pelvic pain on the right side then your diagnosis would be Ilio-Costal Syndrome. This is a well known ribcage anomaly due to a longer 12th rib. Its subtotal removal is the surgical treatment of it that provides a definitive relief of the discomfort caused by it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was wondering about this for a long time. I am 58 years old but the top of my head is a little flat and my forehead is a little high. I am ready for a brow lift but I also wanted to check into possibly when this is done, changing that flatness to the top of my head. I always try to have height when I style my hair due to this look. Very frustrating and annoying to me. My hair is thicker in the back but is not so thick on the top or sides so I need to be careful.
A:The flatness on the top of your head could be augmented to create a more convex shape with a custom skull implant. That could be combined with a browlift procedure. Please send me some pictures for an assessment for this potential combined surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My biggest concern with my hip implants is the edge bending on both sides.
A:That certainly looks like inferior implant edge bending to me. That is a difficult problem to solve in an established pocket. Its best prevention is with the initial implant placement and the placement of ingrowth holes through the implant so the tissues grab onto the implant and provide support to its vertical position. Once the capsule is established you can’t create that biologic effect secondarily as there is no adhesion between the implant and the capsule. The best strategy at this point is to place the implants under the established capsule over the muscle/fascia in which it will be treated like a ‘new’ implant placement. (I would still reduce the implant a bit and place perfusion holes)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about eyes- my eyes look quite round, shallow set and there is scleral show. I would like my eyes to be more hooded and with “straight eyelids” if that make sense. What can be done to achieve this type of eyes? I found on your website examples of supraorbital and infraorbital rim implants with saddle to reduce vertical height of eye socket- do you think those would help to make my eyes more compact and vertically narrow? Would implants improve the canthal tilt? Below I attach the photo of my eyes and eyes which I would like to achieve since photos say more than words plus those examples of rim implants I mentioned. Thank you very much for answer.
A:While I see no attached pictures of you the concept remains the same as you have described…the foundational changes are important to increase bone support above and below the eyelids. In the lower eyelid a canthopexy with a spacer graft is the concomitant procedure to maximize the lower eyelid repositioning effect.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I do my neck exercises regularly everyday with my neck harness. I load with weights between 50 pounds and upwards to 100+ pounds. I have included a video to better describe my neck exercises.
I need to know if these exercises will damage my custom implant or not. Because I really, really do NOT want to ever damage my custom implant. Especially after waiting a lifetime to have my custom implant and all the expenses to get this surgery.
But I also wish to not be unable to do my daily important physical therapy for my cervical spine/neck. I need to regularly do my physical therapy for my cervical spine/neck especially after serious repeated injuries suffered during childhood to my head and neck, which has resulted in the need for this surgery in the first place.
Maybe I’ll have to wait some time after surgery to be able to continue my neck exercises with my neck harness and/or will have to decrease the weight? How long?
Perhaps I will have to PERMANENTLY decrease the weight after surgery? Hopefully NOT, because it’s so satisfying to be able to exercise with heavy weights and progressively increase the weights. But if – unfortunately – yes, then what would be the maximum amount of weight recommend by Dr. Eppley?
A: Thank you for your very thoughtful question. Since your skull implant will be sitting completely on bone and not on or over any muscle (temporal or neck muscles) I do not see any contraindication to doing neck exercises after surgery. I would wait a month before resuming them after surgery to allow the skull implant to fully heal.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, To indicate the type of cheek changes I am looking to make I can only really represent those changes using photos other people that have the features. Essentially, I want to be able to have an ogee curve with the high angular cheekbone look directly underneath the eye which is associated more to a masculine 3/4 profile as well as hollow cheeks that contour as a result? I’m unsure about my facial structure generally and with where it currently stands, are my cheekbones already high but projecting more laterally? is it just that they are not anterior projecting enough therefore cannot replicate the look I’m referring to? What would you advise I do next?
A:You are fundamentally talking about some version of the high cheekbone implant which is designed to create that type of ogee curve change. (see attached) Whether that would have that effect in your face depends on what your face looks like which remains unknown to me at this point.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have some questions about custom skull implants:
1. How big will the scar be and how noticeable will it be? Since I will constantly shave my head.
2. When we reach our goal with the implant, will the result be permanent? Can my skull change over the course of my life and damage the implant? Will I need a second operation?
A: In answer to your custom skull implant questions:
1) The incision is placed low on the back of the head and is less than 7 centimeters in length. It usually heals in a nearly imperceptible fashion. Most patients that have this type of surgery are men who either sgave their head or have very closely cropped hair so our experience such incisions is vast. No patient has yet ever requested a scar revision due to its appearance.
2) Such skull implants produce permanent results that will not change. It is also impossible to ever damage the implant.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question regarding the relationship between hips and obliques and the appearance of hip narrowing/making tiny differences in width of the one oblique on my body. Obviously I know illac crest shaving is a potential option which will slightly pull in the hip which is last resort for me, but I am wondering what are other potential ways to have a similar effect even if tiny? I have a very large oblique muscle on one side of my body (the right) that is overdeveloped due to overtraining and tons of pressure on it for years due to the way I sit, stand, do things, etc , would atrophying that muscle (through botox, radio frequency, or electrocautery) cause it to appear a bit narrower? I know flatter, which is what i’m looking for bc its a large bump but does overdeveloping the oblique make the hip push out more because the bone had to grow with the muscle growth? I’m just wondering if that area of the illac crest and oblique muscle would slightly shrink in length if the oblique was overdeveloped and was atrophied alot. Also if you have any other suggestions to either appear or produce small differences in the length of my oblique muscle/crest, it would make me very happy. I have postural issues and functional issues that cause me to lean in a way that pushes out my right hip/oblique and im assuming seeing a pelvic specialist could make a small difference as well. I”m really looking for just a bunch of small things that could each make a tiny difference.
A: I don’t think there is much of a relationship between hip bone size and the oblique abdominal muscle despite that some of its insertion is onto the outer lip of the anterior iliac crest. Certainly shrinking the oblique muscle will not change the shape of the iliac crest in an adult. The only approach that would produce a positive change would be surgical reduction of the oblique muscle (debulking) and a little shaving of the iliac crest all done through the same small incision. Releasing the attachments of the oblique to the crest will ultimately cause it to atrophy.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Photos and goals were requested for Hip Augmentation.I really need Lipo and hip implants as well as breast implants.
A: The main concept to grasp about hip implants is that they have the highest complication/removal rate of any aesthetic body implant. There are numerous reasons why that is so but awareness of that inescapable issue allows one to understand how to approach hip implant augmentation.
Thus, my first advice would be if someone knows they need liposuction, and it is more than just a spot area, take that fat and first invest it in the hip area. While fat injections is an unpredictable procedure in terms of % survival it is worth that effort because it is complication free from a hip standpoint and one needs the fat removal done anyway. Even if the fat injection results are inadequate it prepares the hip area better to secondarily receive an implant and potentially lower their complication risks.
I can’t speak for your breast implant needs since I don’t know what your breasts look like.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 7 months ago, I had a chin implant and it looks very boxy. I’m not sure what exactly needs to be done to help it. It also makes my mouth move like a ventriloquist dummy and makes the folks around my mouth now prominent.
A:Without even knowing what style and size chin implant that you have I can tell from the outside it is too wide and sits too low on your chin. You need to exchange that for a specially designed v-shaped chin implant that is smaller and is positioned properly on the bone. I would need to see a copy of the operative report from your prior surgery and it would ideally be helpful to have a cone beam scan of your chin which would show the exact position on the bone as well as it shape.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am contacting you because I would like to know if it is technically possible to effectively treat a mild orbital dystopia at this time. I can only find very little satisfactory information on this subject on the Internet. I have a general facial asymmetry, my face is globally asymmetrical, and even though it is not obvious or abnormal, it is in fact unsightly. It’s a complex that I’ve been carrying around for a long time and it’s proving to be psychologically very difficult to overcome. I know it’s a complex and delicate problem, and from what I’ve read on the internet, it’s difficult to treat and rather risky, but I can’t bring myself to give it up. Thank you for taking the time to read me, I hope you have a great day.
A:You are referring to what I call aesthetic vertical orbital dystopia (VOD less than 5mm horizontal pupillary difference) which is neither overly complex to treat nor risky. The pertinent issues with aesthetic VOD are 1) how many periorbital components need to be treated for an effective improvement (orbital floor augmentation alone is almost never adequate), 2) how effective will the procedure be and 3) will any revisions be needed. Preoperative assessment includes a frontal facial picture as well as a 3D face CT scan for treatment planning purposes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am reaching out about a few implants. I am looking to create a more masculine and symmetrical appearance on my face.
From what I can gather myself (I’m no expert of course) I would guess that the infraorbital implants would be the most helpful to my overall face structure, and I am also very interested in a chin implant.
As for the jaw, I am just curious what would provide the most cost-effective symmetry. Do you think a jaw angle implant on my significantly weaker side would be helpful?
I truly appreciate any feedback and your time. I am looking forward to hopefully meeting you!
Info – 24 Y/O Male, have had Radiesse in the chin, cheekbones and jaw.
A: Thank you for your inquiry and sending your pictures. Your face has some significant asymmetry where the right side is overall lower than the left. This accounts for every feature asymmetry that you see from the vertical orbital dystopia (VOD) to the jawline asymmetry. Your lower eyelids also have significant retraction and scleral show. This when looking at infraorbital and jaw enhancements here are the basic concepts:
1) Any attempts at infraorbital augmentation must be accompanied by lower eyelid repositioning with canthoplasties and spacer grafts. With the VOD custom infraorbital implants would be needed to address the bony and eye differences between the two sides.
2) While you can have a chin implant by itself, any efforts at correcting the jaw asymmetry requires a custom jawline implant. Just trying to place a jaw angle implant on the weaker side always just magnifies the asymmetry because the problem is not just in the jaw angle area, it is the whole side of the jawline that is asymmetric. Optimal jaw asymmetry correction requires a complete jawline approach.
Dr. Barry Eppley
Indianapolis, Indian
Q: Dr. Eppley, Thank you for the knowledge you publish on your work. I’m a 24 year old male from Washington DC. I’ve read your answers regarding paranasal implants and premaxillary implants closely to determine what could be the best procedure for my sunken in midface, protruding mouth, acute nasolabial angle, and an upper lip that protrudes beyond the lower noticeably (picture attached). I am concerned that as I age, the upper lip/philtrum will continue to get longer, and due to the acuteness thus contribute to even more protrusion? I am wondering if you can comment on that as well!
I have no malocclusion (had braces + 4 extractions). I originally thought paranasal implants would be appropriate to make a concave midface, which would increase the nasolabial angle/hide mouth protrusion.
However when I found your readings it seems the premaxillary implant, different from paranasal, is best for my situation. I am concerned that a premaxillary implant may make my upper lip protrude further past my lower lip, even if it opens up the nasolabial angle. I am also aware of the risks such as the effect on the smile.
I’m hoping if you can comment whether this path might be appropriate for my protruded mouth situation, and on the concerns of it advancing the upper lip even further past the lower.
A: Thank you for your inquiry and detailing your midfacial augmentation objectives. I am at a major disadvantage when trying to answer your questions since I have no idea what you look like. A description alone is inadequate. In addition the way any facial reshaping procedures are determined is by computer imaging of the patient’s pictures of the various potential changes. As a result any meaningful insight I could provide requires pictures to do these assessments.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, you did such a wonderful job informing me of all the options during my initial consultation and taking time to explain details. Here are a few additional questions for you.
1. How would we determine if I would need vertical lengthening as well as horizontal movement with chin implant in place? Imaging? I have always felt my chin/ lower facial third was too “short” pre-implant.
2. If a very slight V shape is desired, would that require a T- osteotomy in my case or would the genioplasty naturally provide that?
3. Are there potential complications with teeth root damage? How long does it typically take for the teeth tightness to disappear? Any chance of permanent gum numbness?
4. My main motivation for the implant removal + genioplasty is to alleviate overall chin tightness and likely capsular contracture of implant- if the incisional tightness persists post-genioplasty, would the fat graft and release of labiomental fold be a viable option?
Thank you,
A:In answer to your questions:
1) Your are correct in that imaging is the way to determine if any vertical lengthening would be beneficial. I would compare the prior imaging sent to you, in which no significant vertical lengthening was done, with the new attached imaging in which vertical lengthening is added.
2) If you are getting vertical lengthening i would do a T-shaped genioplasty for the sake of a ‘slight’ V shape. That may occur naturally and also runs the risk of added scar tissue and tightness which is exactly what you are trying to treat.
3) There are no potential complications with tooth root damage as the osteotomy cut is well below the tooth roots. Most patients will experience some temporary lower incisor tooth numbness but that is not due to root damage.
4) Your secondary plan for persistent chin tightness is the appropriate one with the highest change of success.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m 43 y.o.and all my life I’ve got complex about my deep set small eyes. I’ve seen your answer on your website about it and that make me write to you Dr.
When it comes to trying to improve deep set eyes, there are few options. You can not move the eyeball forward by any method, all that can be done is to reduce the surrounding orbital bone along the brow ridge and the lateral orbital rim. Depending upon the prominence of the brow ridge, this can be particularly effective. It is important, however to separate the terms ‘deep set eyes’ and ‘hollow eyes’ for they represent different orbital morphologies. A deep set eye is when the globe (eyeball) sits far behind the surrounding orbital rims, particularly the superior and lateral orbital rims. Reducing the projection of the surrounding overprojecting bone is what can make the eye seem to come forward. Conversely, a hollow eye appearance implies that the relationship between the globe and the surrounding orbital rims is normal but that there is a lack of fat in the lid areas, having them retract posteriorly. The hollow eye or lid deficiency/retraction can be treated by fat injections.
And is any change I could have it done ?
A:Thank you for your inquiry and detailing your periorbital concerns. The first place to start is to have me look at some pictures of you, particularly the side (profile) and oblique views, in which computer imaging can be done to see what type of periorbital reduction can be accomplished in your case.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m considering a custom jawline implant and have a few questions. I live in Montana so could the initial consultation be virtual? I also have a short to medium length beard and would really rather not shave before the surgery so would I need to shave or trim my beard for the consultation? How long would recovery time be before swelling would go down? And when would be the soonest I would be able to have this procedure done?
Thank you
A:In answer to your jawline implant questions:
1) All initial consultations are done virtual.
2) In designing a custom jawline implant it is important to do computer imaging to determine the patient’s specific goals. Having a beard that makes the jawline completely invisible makes that challenging/impossible. The other option is to use the bone (3D CT scan) and make the design based on the bone deficiency that I would need to interpret.
3) The design and fabrication process (getting the implant ready for surgery) typically takes 3 months so that provides a base timeline for surgery scheduling.
4) Recovery is largely about swelling. While its entire resolution takes months, most people look reasonable in 2 to 3 weeks after surgery.
Dr. Barty Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had custom jaw/mandibular angle implants installed by another surgeon. My right and left sides naturally had some asymmetry, the left a fair bit more deficient. The right implant worked out well, but the left came loose and shifted forward. The surgeon performed a revision on the left. He shaved it down a little bit and placed it once again, this time with bigger screws. But it looks like it has shifted a second time! The implant isn’t super ambitious in size at all so I’m wondering what my options are? Is it reasonable to try again? Should I go to a different surgeon? Is there anything else my surgeon can do to guarantee it doesn’t shift again? I’m quite distressed and I know Dr Eppley is a master of the field so I’m just looking for any answers or expertise he can share. I feel like I should have gone to him to begin with!
A:What you need to answer your question is three pieces of information to provide a qualified opinion:
1) Before and after patient photos
2) The original implant design file
3) a current 3D Ct scan of the lower jaw
Any comment or decision made on less than this information would be an uninformed one.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m a 32 years old male. Since a long time I’d like to reduce my temporal head breadth a bit and I was also never satisfied with my too wide cheekbones.
As for this matter, I had a cheekbone reduction in January 2020 in South Korea, and I’m not 100% satisfied with the result. Especially after the screws came out. It’s still a bit too wide, especially at the end of the zygomatic arch near the ears I got some small “bulges” which I hate! It’s probably a mix of scar tissue and bone. Unfortunately, I can’t reach the Korean surgeon anymore for a post-correction.
I’m very unsatisfied with this and would like to consult Dr. Eppley for this matter. On photos or video, it’s very difficult to see what I mean. As far as I understood, he offers these kinds of operations and hopefully could bring the result to a satisfying finish for me.
For this a personal meeting would be important for which I could bring the current 3D DVTs (digital volume tomography).
I’m looking forward to hear from you.
A:What I need to see is a postop 3D CT scan. Most likely this represents a prominent posterior zygomatic arch which has either not been reduced or continues to have a prominent arch shape to ir which is very common.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 2 questions for you how much would a mouth widening procedure cost? Also, would you have any idea what’s “wrong” with my smile? I’ve scoured the internet looking for similar smiles and answers to what could be causing it too no avail. My smile looks kind of “forced” and wonky. Could it possibly be paralysis of some sort? I also get tightness in my chin when I smile, chin ptosis perhaps? I’m at a loss as too what could be causing my smile too look odd. I attached 2 photos. 1 of me smiling and one of a smile I’d consider more normal I guess. You can see that mine looks forced and uncomfortable and his looks natural and relaxed. Thank you in advance dr!
A:You have overactive depressor lip muscles and poor excursion of the lateral upper lip elevator muscles, creating a forced or abnormal mouth shape when smiling. There is no surgical solution to that facial muscular activity. You can always try Botox to the lower lip depressor muscles and see if that helps. I would not be certain that mouth widening would provide much benefit for your smile.
Dr. Barry Eppley
Indianapolis, Indiana