Your Questions
Your Questions
Q: Dr. Eppley, Also, want to double check that, given the clavicle(s) have had adequate time to heal, I should be able to resume heavy weight workouts–I am benching and rowing above 200 lbs multiple times per week, definitely not power lifting, but also potentially putting more strain on the clavicles than is standard. Not sure if these particular exercises would even be the ones I ought to be concerned about, but yeah, wondering if its possible to get some reassurance that this operation shouldn’t limit my ability to workout (again, assuming adequate time is allowed to heal the clavicle(s))
Thanks!
A:Provided adequate time is given for full bone healing, there should be no restrictions for those activities after clavicle lengthening surgery.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in consulting about getting chin and jaw implants. When I was six I had cancer and extensive radiation delivered to my facial region resulting in a stunt of growth in my mandible.
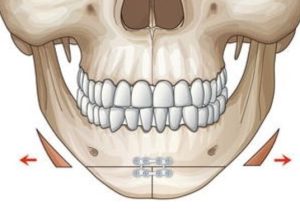
Q:Thank you for your inquiry and sending your pictures. With the history of radiation in the area we have to be very cautious about treatment selection as that affects the involved tissues lifelong and their ability to respond to trauma and exhibit normal healing from it may be compromised. (at the least it has a higher risk of infection) I will need to see a 3D CT scan of your lower face (jaw areas) to have a better appreciation of the bony anatomy. With the history of radiation a custom wrap around jawline implant is out as the infection risk is too high. Thus, for now, I am thinking a bony genioplasty (you need mainly vertical lengthening anyway and jaw angle implants. The bony genioplasty will be fine, it is the jaw angle implants in the back we have to assess very carefully.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Here are some of my desired results from rib removal.
Waist: 28-30
Hips: 40
Inseam: 32
I really want that golden ratio of a .6 waist to hips. I think that a 26-27 inch waist with a 42-44 inch hips is a buffer. Here are photos of what I would like, I will attach photos of myself currently, with as little fat and showing abs for best results.
A:Thank you for your inquiry and sending your pictures. I think with your lean body frame the only way you are going to have a more narrow waist is with rib removal surgery. How much waistline reduction you can achieve with this surgery is never completely predictable so I would not specifically provide a waist measurement number for what can be achieved. The only outcome aspect of rib removal surgery that is assured is that once this is done there are no longer any further anatomic reductions that can be done. Rib removal surgery is the last stop on the waistline narrowing train.
Dr. Barry Eppley
Indianapolis, Indiana
 Q: Dr. Eppley, Is such a skull implant possible for women with no effect on hair color and heat on it ??
Q: Dr. Eppley, Is such a skull implant possible for women with no effect on hair color and heat on it ??
A:Correct, the implant material only changes shape/breaks down at 375 degrees F.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Questions about how to correct a sloping forehead with a very strong low brow bone with temporal hollowing.
A: That would be done with a custom forehead implant (minus the brow bones) that has temporal extensions.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I live in Sweden and I’m interested in cheek augmentation for the high cheek bone look. The thing is I’ve done an operation with cheek augmentation here in Sweden (intra-oral) but I didn’t get the high cheek bone result.
Is it possible doing this operation , going through the lower eyelid as shown?
A: There is no standard form of cheek implant that can achieve the high cheekbone look…which is largely a horizontal augmentation along the zygomatic body and arch. Whether that would also include the more anterior infraorbital rim is determined on an individual case basis. Most of the time the preferred method of accurate implant placement/positioning is through the lower eyelid.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, I was looking into forehead contouring surgery to reduce frontal bossing and had a few questions that I hope you can answer:
What is the average cost for forehead contouring to reduce frontal bossing?
How are nerves and expressions affected after the surgery?
Does the hairline look natural after patients are fully healed and what’s the recovery time?
When you start shaving the bone, are you making the bone super thin and is that dangerous? Or does frontal bossing create a thicker layer of bone that can be shaved down to a normal thickness. If that could be explained, I’d like to know.
I’m looking for information to get started, but there’s not much to go off of online, and all the info varies greatly. Any help would be appreciated. Thanks
A: In answer to your forehead contouring questions:
1) My assistant Camille will pass along the cost of the surgery.
2) Some temporary numbness of the front part of the scalp and forehead stiffness will occur right after the surgery…all of which resolves in a month or two later.
3) The key question in approaching the upper forehead is whether a hairline incision is used or whether it is placed behind it. But most hairline incisions heal well and look natural provided one has a good initial hairline density.
4) To determine how thick the forehead bone as it relates to the frontal bossing a preoperative x-ray is taken to determine its thickness and see how much bone can be safely reduced.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Also I got a rhinoplasty and chin implant and lipo done several days ago. But I would like to do more lipo (I believe you call it a buccal myectomy) and custom implants that might replace the existing chin implant if required. How long should I wait before getting another procedure done?
A:Three months after the last procedure would be sufficient. If a custom chin implant is needed for a replacement for the standard chin implant just done now would be a good time to get started since that will take 3 months to design and have ready for surgery.
Dr. Barry Eppley
Indianapols, Indiana
Q: Dr. Eppley,Hello. I love your work. It is so wonderful to see a surgeon that is so talented and passionate about the outcomes of every procedure.
I wanted to ask in regards to a sliding genioplasty in your experience what is the risk of severe bleeding during and post operatively on a healthy patient that does not take any medications.
Thank you.
A: Of the potential risks and complications of a sliding genioplasty, severe bleeding during surgery or a postoperative hematoma is not one of them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I know after shoulder narrowing surgery patients are released for full activity after 12 weeks but what is your recommendation for returning back to work? (more range of motion at weeks 5 and 6).
A:That is probably not unreasonable. Given the type of work a dental assistant does the range of shoulder motion at one month after the surgery should be adequate.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, So as you can see i have a certain eye area that looks nothing like my desired result (below), and i would like to know the best and most efficient surgeries and augmentations that would take me from what i have to something with the same characteristics as the model below. (a Fair amount of Hooding, 0 sclera exposure and positive canthal tilt). Also it might not be visible in the photo, but i also have a negative orbital vector that is especially striking whenever i squint or lift my eye.
A:I would say the major difference between you and the model eye look is that you need a lateral canthoplasty, spacer grafts to the lower eyelids and infraorbital-malar implant augmentation for the lower orbital area. The upper orbital area needs filling of the supratarsal area with some form of a fat graft. (fat injections or an en bloc fat graft) Your brows seem to be sufficiently low.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a rhinoplasty done 5 years ago to correct the contour of the sides of my nose. While the surgery made a very significant improvement, the left side is still a little curved from front view, while the right side is straight. I met with a different surgeon recently about whether or not a non-surgical liquid filler could correct this issue, and they said they wouldn’t recommend injecting a filler after a previous surgical rhinoplasty, as it’s “a little dangerous”.
I’m not sure what the danger is they’re alluding to, but if it’s the vision loss I’ve read about, and the risk is high enough, it might not be worth it. If the risk is very low, though, maybe it would be worth it.
A: If the goal is to augment the flatter side of the nose to better match the curved side, then the use of injectable fillers is a reasonable non-surgical approach.
When it comes to the use of injectable fillers in the nose the risk to which is being referred is that of an ischemic event. This means the pressure of the filler causes a compression of the blood supply to the overlying skin resulting in an area of necrosis or eventual skin loss. In the scarred nose (prior rhinoplasty) this risk is higher due to this scar tissue. How significant that risk is can be debated but I can’t fault the surgeon from passing on doing it as for him/her the reward:risk ratio is just not worth it. Its occurrence may be uncommon but it would create a deformity worse than the original aesthetic problem.
Dr. Barry Eppley
Indianapolis, Indianapolis
Dr. Eppley, Do you perform mouth widening surgery and do you feel it can be done with acceptable scarring. Conversely is there an alternative surgery that can achieve this. My goal is to widen my mouth and smile.
A: Mouth widening is a procedure that I essentially developed from an aesthetic standpoint. Whether the scarring is acceptable is a matter of individual interpretation. What is an issue not open to interpretation is that the need for scar revision in mouth widening surgery is 50% or greater.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I hope you are well. I have a few questions regarding the clavicle lengthening procedure I have scheduled with you in June and was hoping you’d be able to help.
The first thing is regarding a potential complication. It appears I may have either a Type 1 or Type 2 acromioclavicular joint injury (I’ll attach pictures). I don’t recall any particular trauma, and it may have just been caused from weightlifting over time, or by something that I didn’t think was painful enough to seek out medical attention or suspect an injury. Either way, this was taken a few months ago and it appears to be the same (no further healing). From what I’ve read (but I may be incorrect of course), it seems that if a few months has passed and the injury persists, it likely will not heal on it’s own. I’m curious if you think this is any reason to be concerned when planning lengthening of the clavicles.
Although it is not causing me trouble now, I’m not sure if it may need to be corrected by surgery if it gets worse (or possibly now to prevent it from getting worse). If you think clavicle lengthening is still feasible, would you think it may cause any complications to a potential A/C joint repair in the future? I ask because I wonder if this is something best corrected now, or if it can probably wait until later (if needed at all) after a recovery from clavicle lengthening. I just wanted to make you aware of this before my X-rays the day before surgery, and to get your opinion.
The second question is regarding exercises and preparation for surgery. Since the lengthening procedure will stretch some muscles, I would imagine it would be beneficial to stretch affected muscles as much as possible beforehand. Would you think this is a good idea, and if so, would you be able to provide a list of muscles that I should be stretching?
Thank you for your time and insight.
A: In answer to your questions:
1) I am not an AC joint authority but I don’t see the correlation between a lengthening osteotomy done on the inner third of the clavicle to whatever injury exists at the distant outer joint. The clavicle bone is of good bone stock so I see no reason why it would have any trouble healing.
2) The reverse question seems more pertinent….how does a lengthened clavicle affect an injury at the AC joint? That is a question outside my field of knowledge but I would think important to know. This would have to be answered by an Orthopedic Shoulder Surgery specialist.
3) I would certainly see no harm in any shoulder strengthening or stretching exercises before surgery…although I can say they are absolutely essential. The amount of clavicle lengthening achieved in the surgery is not going to be limited by the natural flexibility of the tissues. But I think it is always a good idea to ‘train’ for body surgery almost regardless of what that surgery is.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had orbital floor surgery on my right side for a fracture. I do some acting but feel I lose parts because my eyes are no where symmetrical. I think the surgery was rushed leaving my replacement floor on my right higher than my left. Thoughts?
A: While I don’t know what you looked like before the injury and before the surgery, and your face is a bit tilted in this picture, the eye asymmetry is obvious. (see attached) It is clear the right orbital floor reconstruction is higher then the left unaffected side. That can be remedied but a 3D CT scan should be done first to have a precise measurement of the different orbital floor heights. That would then be matched with the differences in the external horizontal pupillary levels. (which presumably is 1:1 with the differences in the level of the orbital floors. Do you know what material was used to reconstruct the orbital floor?
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I workout 6 days a week and it seems that no matter what I do it’s hard for me to get any real definition in my pecs. I have a very broad chest. I’m 6ft 3 and weight approx 208 lbs. I would be curious if I could get the results I’m wanting for my build with a standard implant or if we would need to go custom to get an idea of $. I have attached a few pictures for reference. Please let me know if you have any other questions.
A: The decision between standard vs custom pectoral implants comes down to what your augmentation goals are in the amount of projection as well as your muscle measurements. (height and width, see attached image) If I could see some examples of your pec augmentation looks as as well as these measurements I could answer what type of pectoral implant would work best for you.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had facial feminization surgery with very bad results. My chin was amputated instead of contoured or a genioplasty. My mandibular angles were totally obliterated too. This has left my face looking unnatural and with a U shaped. My chin pad hangs below my chin bone now.
I’m interested in Rib reduction too as i have a rather straight waist, very short torso, 5’7″ tall, ~30″ waist inspite of being thin due to being born a man (I transitioned 3 years ago)
Question:
My question is can my ribs be reduced by a couple of inches?
Can the rib bone be grafted to make my chin better and give me some mandibular angles. (Even if only a slight augmentation is desired)
Even if rib reduction is not possible can I still get a rib bone or other graft to make my facial harmony better? Im also scared of losing more bone as I age and having danger to my teeth.
Attachments:
I have enclosed CT scan images post op and can provide complete ct scan zip folder too.
Please do help, if possible. After all this I still look male in person.
My main concern is my face shape, and I’m terrified of choosing implants as I barely have a few mms of bone left in my chin.
A: Thank you for your inquiry and sending your 3D CT scans. Like all 3D facial CT scans they speak for themselves about the state of your chin (an amputation chin reduction is a very unusual procedure given the objective) and the not atypical amputation of the jaw angles in V line surgery. (albeit with a very high starting point to begin the bone cut)
While custom implant designs are the far superior method of subtotal chin and jaw angle reconstruction after any form of V line surgery, and there are no long-term bone loss issues with such implants, your question of whether bone from rib removals can be used for the chin and jaw angle reconstructions is a logical and reasonable one.
The length of ribs removed varies depending upon which rib is being taken. Rib #12 is usually in 5 – 6 cm range, and ribs #11 and #10 are in the 10 to 12 cms range. Such ribs are usually 1.5 to 2 cms wide. Given these bone lengths their additive amount should suffice for the chin and jaw angle reconstructions.
The issue with using rib bone for the chin and jaw angles, and this applies to any bone graft on the jawline whose objective is to expand the existing contours, is how much of it will survive. Onlay bone grafting can have different volumetric fates than inlay bone grafting in the face.
But the recycling of bone from rib removal instead of merely being discarded is not completely novel. Its most common recycled use in my experience is in augmentative rhinoplasty.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I just want to clarify that after the surgery, once the clavicle is healed and strength restored, the procedure can be done again, this time lengthening both clavicles. It is my understanding that a clavicle lengthening procedure can be done more than once as long as adequate healing time is given in between. My end goal is to have the right clavicle lengthened twice, and the left lengthened once.
A: That is a correct concept. The clavicle is a very robust healing bone and as long as it is fully healed and has a normal cross-sectional diameter, the lengthening osteotomy can be repeated.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, The left side of my face appears entirely flattened and hollow. My forehead is hollow on the left, my left cheek bone is pushed in, my left jaw is flattened, and my lip is also misaligned. My eyes are also uneven (one smaller than the other) due to plagiocephaly, and my nose tilts and sinks in towards the left side of my face
Therefore, what surgical procedures could improve the deformities mentioned above?
A: Based on this description alone the possibilities include:
Left Custom Forehead/Cheek and Jawline Implants
Left Paranasal Implant
Rhinoplasty ??
Upper Lateral Lip/Mouth Corner Advancement/Lift
Hard to say about the smaller eye without seeing pictures.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had cheek implant removed a year ago along with chin implant, wondering how long it takes for the implant capsule to fully go away or if it will fully go away, it was a silicon implant that was only in for 8 months.
A: Facial implant capsules take 6 to 12 months to be completely absorbed.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I suffer with chronic infections at the corners of my mouth, due to saliva tracking there, I wanted to ask my dermatologist if surgery was a option, as summer approaches when I suffer the most. I`m concerned my insurance will consider it cosmetic. At this point, I`m just asking questions. (I`m 71 and live in California, I realize you`re in Indiana)
A: It is fair to say that with your very downturned mouth corners which causes an overhang, this is a frequent cause of angular cheilitis. The mouth corners need to be lifted to remove the overhang and not allow the moutb corners to be chronically wet.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Would it be unwise to undergo total periorbital augmentation, potentially including the zygomatic arch, PRIOR to orthognathic surgery in both jaws? I suppose this is an issue mainly for the infra orbital rim part of the implant design process. The aesthetic concern is, for the most part,vertical deficiency that results in round, saggy – retracted lower eyelids as shown in attached photos. However, since some degree of horizontal augmentation may be necessary, wouldn’t that impact either the implant design process with you or the surgical planning with the maxillofacial surgeon?
Thank you in advance.
A: The level of a LeFort I osteotomy is below the infraorbital rim (technically below even the infraorital nerve) As a result, periorbital augmentation and orthognathic surgery are done at two different facial bone levels. Thus their order of execution is more of an aesthetic choice. While it may seem that one area affects the other from a treatment planning standpoint, it does not.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I noticed that your clavicle lengthening results usually add about two inches overall. Since the pectoral muscle attaches to the clavicle does this usually result in a broader chest?
A: Your supposition would be correct. As the clavicle is lengthened it pushes the shoulder out. Since the insertion of the pectoralis muscle is attached to the humerus (upper arm) it will also get pushed out laterally. This will move the lateral pectoral muscle border, which is what defines the width of the chest, outward. Thus the chest does get wider as the clavicle gets longer.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I have dynamic/ hyperdynamic chin ptosis. I‘ve planned to get a V-line Surgery in Seoul in some months, where the blunt and wide tip of the chin is cut off by osteotomy, and unnecessary bone parts are cut out, which are reassembled at the bottom center. My question is can I have the surgical treatment for dynamic/hyperdynamic chin ptosis afterwards? I would like to get both surgeries done.
Have a nice day!
 A: I am very familiar with that form of mini V line surgery since I frequently perform it myself. There is no question that hyperdynamic chin ptosis correction should be done AFTER this surgery since the loss of supportive bone structure will make the hyperdynamic chin ptosis worse. Or if done before would eradicate any positive benefit from the hyperdynamic chin ptosis correction.
A: I am very familiar with that form of mini V line surgery since I frequently perform it myself. There is no question that hyperdynamic chin ptosis correction should be done AFTER this surgery since the loss of supportive bone structure will make the hyperdynamic chin ptosis worse. Or if done before would eradicate any positive benefit from the hyperdynamic chin ptosis correction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Question about how to correct a sloping forehead with a very strong low brow bone with temporal hollowing.
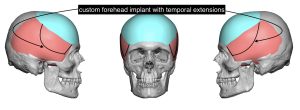 A: This is a not uncommon forehead shape seen since it is reflective of an overall more narrow skull shape in an anteroposterior direction. Because you are a male your brow bones developed normally but what has developed around them is less developed. This would be effectively treated with a custom forehead implant (minus the brow bones) that has temporal extensions. (see attached)
A: This is a not uncommon forehead shape seen since it is reflective of an overall more narrow skull shape in an anteroposterior direction. Because you are a male your brow bones developed normally but what has developed around them is less developed. This would be effectively treated with a custom forehead implant (minus the brow bones) that has temporal extensions. (see attached)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am contacting with regards to my request for a virtual consultation.With this message I want to outline my concerns/expectations in detail since that wasn’t possible with the other form.
1) My primary wish is to improve the lower third of my face (chin, jaw). By that I mean:
a. Making it more massive, increase it’s overall size. My lower face should take up a bigger portion of my face. I have gained a lot of muscle mass these past years (and some fat mass as well). Also I am about 6’2. That means I am a really big guy and my face doesn’t quite match that (it’s not narrow or rescinded, it is about average and that’s no longer enough). My jaw needs to be much wider and have a wider angle. Also my chin needs some more projection. That way my lower face would fit in better with my overall physique. It is very important to me that the surgery does not end up being barely visible, it should be clearly noticeable, ie the implants have to be massive enough. I found several great before-after improvements in your photo gallery “Custom Facial Implants” that we should perhaps lean on for my own implants. Those are the transformations of patients “1”, “2”, “48”, “54” and “56”.
b. Making it more defined, more “chiseled”. A big part of this could be simply decreasing my overall body fat percentage though. Perhaps neck liposuction could be helpful as well since I definitely have a certain fat pad below my chin.
c. Add either a cleft or dimple to my chin. This is purely a preference of mine and I believe the facial implants are a great opportunity to check that off my list too.
2) Another goal of mine is to improve on my facial (a)symmetry. I don’t know exactly how to achieve more symmetry, I guess the facial implants are one way, maybe they are other procedures to improve symmetry as well that you could inform me on.
A: Thank you for your inquiry and detailing your objectives to which I can say the following:
1) How large any facial implant can be is a function of the soft tissue tolerances to which is placed underneath them. Thus there are limits which must be made on an individual basis.
2) Chin clefts and dimples do not come from indentations in the bone. Therefore putting those features into an implant design will not necessarily make it appear on the outside. These are soft tissue muscle defects which, in large chin/jaw implants, may not be wise to do since this requires thinning out the soft tissue over them.
3) Whether midface (cheek) implants may be necessary for facial balance/proportion with a larger lower third jawline implant augmentation will require computer imaging to assess.
4) At age 20/21 99% of your lower jaw growth is over so there are no concerns with implant placement.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Do the temporal shell implant last forever and how much does it cost? Thank you for answering in advance.
A:The temporal implant is made of an ultrasoft solid silicone material that does not degrade or break down. It can only changes its chemical structure at 375 degrees F. Thus it will last forever.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley,Hi, I understand your practice specializes in custom facial implants. I have a cosmetic bony deformity from trauma and I would like to learn about your experience with the outcomes of those specific implants and complications, planning procedure, choice of material, etc. Thanks
A: Thank you for your inquiry and sending your 3D CT scans. What you had is a classic ZMC fracture with downward and inward rotation. Unfortunately the ORIF surgery failed to adequately derotate the ZMC complex so there is undoubtably some flatness of cheek projection extending out onto the zygomatic arch. Your two options secondary reconstructive options at this postop time period is a ZMC osteotomy with replating into a better anatomic position or a camouflage technique overlay technique using a custom implant design. Each option as its advantages and disadvantages. The custom inmplant overlay technique oiffers a less invasive surgery with a more assured anatomic restoration. Custom implant designing works just as well in secondary facial trauma patients as it does in aesthetic facial surgery. From a design standpoint it is ‘easier’ than aesthetic facial enhancement use because there is a well defined target. (the opposite normal side)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is there any way to reduce the width of the forehead?
A:Yes there is. It is known as temporal line reduction….the bony anatomic lateral birder of the forehead.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My question is about the possibility of ribcage expansion + pelvic narrowing + clavicle lengthening to create a bone structure for the optimal “V-taper look”, that is desired by many bodybuilders. I notice you already answered a similar question (https://www.eppleyplasticsurgery.com/ribcage-expansion) But i am asking again in the case of any new technological developments.
Compare the image provided. Would it be possible for the left’s clavicle to transform into the right? Or, do you think rather the right’s picture has more of a camera angle illusion, perhaps flexing his lats to create more of a V-taper compared to the unfortunate shoulders of the left.
Do you think it would be possible to undergro ribcage expansion + claviacle lengthening + pelvic reduction with smaller, mini Distraction osteogenesis devices getting released?
Have you ever completed any pelvic narrowing/waist narrowing procedure on men who desired the small waist, V-tape look? If so, what methods were needed to achieve their desired look?
A:In answer to your questions:
1) Clavicle lengthening osteotomies is a real and effective procedure. For now it is done by a sagittal split technique. Distraction osteogenesis with acceptable devices and limited scarring does not yet exist.
2) Ribcage expansion is not a real or even safe procedure.
3) Iliac crest reduction is an actual procedure which may be combined with rib removal of the goal is a very tapered waistline.
Dr. Barry Eppley
Indianapolis, Indiana