Your Questions
Your Questions
Q: Dr. Eppley, My philtrum length is roughly 1.7 – 1.8cm long, and so I think I would be an ideal candidate for a lip lift. My concern is that having the procedure would deform my nostrils. I have attached both side profile and front on images of my face. My nostrils are already quite prominent. I read that minor change in the nose can be a very real side effect. I was wondering whether it was likely the procedure would alter my nose for the worse? I have also heard of vermillion advancement surgery, but I’m unsure as to whether this shortens the philtrum length to give a lifted effect (which is my main reason for the surgery). Could you provide insight here? Thanks a lot.
A:While nostril distortion is not a side effect that I have ever seen from a subnasal lip lift, that risk is undoubtably dependent on how much upper lip tissue is removed as well as the surgical technique used to do it. (wrapping the excision/scar line around the nostrils is a sure way to potentially distort the nostrils) But the way to avoid that risk completely is a vermilion advancement which is also a more complete procedure as it changes the entire vermilion exposure from one mouth corner to the other. Men do exceptionally well with this procedure from a scar standpoint because of their beard skin. You are not an ideal candidate for a subnasal lip lift because of your thinner upper lip at the sides in which an isolated fuller central upper lip may create a A frame deformity appearance.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m looking at the website, but it’s not like most plastic surgeon websites. Does the doctor actually perform the surgery? Or does he supply the custom implant to a surgeon of my choosing?
A: I assume you are looking at www.eppleycustomfacialimplants.com in which after 1,000 custom facial implants performed I show the many different types of types and styles that are available and in which I have done. I do not design or supply custom facial implants to other surgeons.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’m currently undergoing orthodontic treatment for a Lefort I + SARPE surgery in the future. I have a class 3 malocclusion. This surgery should help (though not completely fix my bite). The lower portion of my maxilla is very narrow, and my mandible has shifted and become asymmetric so that my molars connect. However, it’s really my entire maxilla which is quite recessed, and not just the lower portion. I have a very/flat recessed eye area as well (hardly any cheekbones). I’m concerned that a lefort 1 is not addressing the whole problem, and really won’t do much to help me cosmetically. I have been researching lefort 2 as an alternative, but can hardly find any surgeons who perform this operation in the USA. Since I came across your site in my search, I was wondering if this is something you offer. Thanks for your time.
A: When the entire midface is recessed a Lefort I osteotomy, as you have correctly surmised, will provide an incomplete aesthetic correction. By only addressing the dentoalveolar part of the problem the nasal base is primarily aesthetically improved. Anatomically a LeFort III osteotomy provides the most complete correction. (although limited to the sagittal plane)
While more anatomically complete there are quite a few differences (tradeoffs) between a LeFort I and III osteotomies. The latter requires eyeid incisions (technically a coronal scalp incision is more ideal) and osteotomies across the orbital floor and cheek areas. These invariably heal with irregularities and some palpable bony stepoffs. In contrast the LeFort I is a far more aesthetic operation with an intraoral approach only with no evident bony stepoffs.
While LeFort procedures above the I level may be appealing in diagrams, there are aesthetic tradeoffs with their use that are not obvious in such drawings and should be very carefully considered and undertaken with caution. There is a reason they are primarily used in younger syndromic patients with more substantative bony deformities.
While these LeFort II and III procedures can be done in the highly motivated patient a more prudent and effective approach is to employ both a LeFort I osteotomy with custom midface implants above it, either done concurrently or staged.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, how much clavicle lengthening in shoulder widening surgery is safe?
A: t is not a question of safety but what the regional anatomic limitations are. The amount of clavicle lengthening that can be achieved on each side is 20mms. More lengthening would still be safe but the attached shoulder and scapular tissues will not let the clavicle to be pushed out further. (I have yet to see a patient who can get beyond the 20mms as I would love to get 25mms per side)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested in making my brow bones more symmetrical, especially in bringing the higher brow to a lower position, can this be done through custom brow bone implants, and I don’t want to have to raise the position of the lower brow because I think it is more aesthetic than the higher one. I have attached my pictures. I’m waiting for your reply.
A: It does appear that your left brow bone is smaller than that of the right which would explain the higher eyebrow on the left side. Because of the underlying bone asymmetry it may be possible to lower the higher eyebrow with an implant design that makes a better structural match to the other side.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have read online that I could wear a garment to improve outcomes of rib removal waist reduction? Will that help? I need some curve!! And for shoulder reduction when can I get back to the gym for lower body then upper body/ do a push up like yoga?
A: Compression garments, like real corsets or even shapers, can only benefit rib removal surgery in the short term by helping reduce swelling earlier and providing ideal soft tissue shaping. So am I am for their short term postoperative use. More compression is better than less as long as it is tolerable.
For shoulder reduction surgery it will be at least 8 weeks before more strenuous upper body work can be undertaken.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had PMMA cheek and chin implants placed 6 years ago. I’m looking to go the custom route now to address the asymmetry caused by the implants. As such, I have a couple of questions:
– Can the PMMA implants be removed easily without damaging soft tissue?
– Will the existing implants make it impossible for new implants to be designed? Do they have to be removed first?
Thank you!
A: In answer to your facial implant questions:
1) Since the bone nor the soft tissue bonds directly to PMMA their removal should be successfully done. However whether there is bone overgrowth on them, or more importantly, bone resorption under them (most relevant to the cheeks in which there may be maxillary sinus exposure on their removal) it would be important to know what the surrounding bone looks like by a preoperative 3D CT scan.
2) As a general rule I don’t find the need to first remove any facial implants for either custom facial implant designing or their placement. But the need for a preoperative 3D CT scan remains to have more insight into the indwelling implants and the tissue reactions around them.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, . I would also like to know if it is possible to have the clavicle lengthening procedure performed more than once in order to further widen the shoulders?
A: Theoretically clavicle lengthening can be done again…but no one really knows for sure since it has never been done yet.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I designed a custom implant prototype on a 3D modelling software called Tinkercad. I designed a nose implant prototype and a jaw implant prototype. The files are .stl format and I would like to send them to you for viewing. I would like to know if the implants are possible to instal over my natural nose bone and natural jaw bone using a custom silicone implant? The .stl files don’t account for dead space and don’t include a facial x-ray for exact measurements, so I will have to work on it with you. I have had previous work done. I have had 2 modest nose jobs in my home town. I have also had a standard chin implant installed, as well as chin and jaw filler. These need to be removed prior to surgery. My goal is to fully customize my surgery so I don’t have to keep getting work done without a clear end goal and so I don’t have to keep injecting filler which my body metabolizes very quickly. My goal is to have a more symmetrical face and a face that meets the rule of thirds of facial aesthetics.
A: As a general statement your designed nose and jaw implants are guidelines for doing formal custom implant designs done on your actual 3D CT scan. Your general implant designs are not going to fit your existing bone structure. But I would be happy to look at what you have designed so far.
As another general statement the nose is not a very good place for implants unless they are small and restricted to the nasal dorsum. It is a thin tissue coverage areas which means an excessive pressure placed by implants are going to cause complications.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have several questions about iliac crest reduction such as:
local or general Anesthesia?
What is the timeline for healing?
What can i expect immediately afterwards?
What are the long-term effects 10-20 years down the line?
Will the bone grow back?
The photo attached is not mine but very comparable; basically wondering if there’s a way to rip off bone off my Iliac crest in order to get a smaller male hips.
Thanks
A: In answer to your iliac crest reduction questions:
1) The procedure is done under general anesthesia.
2) Full recovery will take up to a month after surgery.
3) Swelling and discomfort is what you can expect right after the surgery. It is akin to harvesting a hip bone graft…only on both sides.,
4) There should be no adverse long term effects other the residual fine line scars to do the procedure.
5) The bone can not grow back.
6) Based on the attached picture the best approach to reduction of the iliac crest hip area would be a combined iliac crest bone reduction with liposuction done in and around the area.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi. How much lengthening of clavicle is possible at max? What are the limiting factors of extension?
 A: In my experience to date the maximum amount of clavicle lengthening is 20mms per side. The limiting factor is that in lengthening the distal clavicle after the osteotomies it is pushing against all of the shoulder joint attachments particularly against the acromion and coracoid processes of the scapula. Whether preoperative shoulder stretching exercises will improve the mobiity of the scapula and make the shoulder more ‘loose’ is yet unknown but I advise my patients to do so.
A: In my experience to date the maximum amount of clavicle lengthening is 20mms per side. The limiting factor is that in lengthening the distal clavicle after the osteotomies it is pushing against all of the shoulder joint attachments particularly against the acromion and coracoid processes of the scapula. Whether preoperative shoulder stretching exercises will improve the mobiity of the scapula and make the shoulder more ‘loose’ is yet unknown but I advise my patients to do so.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am a huge fan of your work. No other surgeon seems to actually listen to what his clients actually request – and also thinks out if the box. I wonder whether you may be able to comment on my recent chin implant that I had performed.
I really wanted a very square strong masculine chin. After I did all the research myself, I convinced the Implantech agent to import a Terino Type 2 implant. Believe it or not the plastic surgeons here are completely unknowledgeable about the different types and none of them do jaw angle implants. The implant was placed intra-orally. I think it was the size L.
To be frank, I am disappointed in the result – there is absolutely no obvious squareness to the chin. I think the outline is there -but it may simply be that the fat pad was not shaped or draped around the chin so as to make the outline of the implant clear.
Only afterwards have I read some of your comments that the Terino implants are NOT necessarily the right type for a square looking chin – and that you favour a custom-made implant.
I have included some pics so that you get an idea of my results. I also attach a pic of what I was HOPING it would look like.
Please could you advise me on what you may be able to recommend for me. Is there any way that you could custom design an implant for me? Could the custom implant be sent to me for the surgery here (as travel internationally has become a HUGE drama).
I would really appreciate any advice you could give me Dr Eppley. I would be very grateful
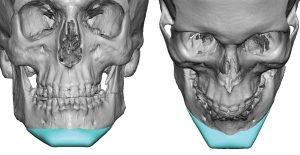 A: As you have pointed out I have never found the standard square chin implants (Terino style 1 and 2) to be very aesthetically satisfying. They have rounded corners, which are wider than the rounded anatomic chin implant styles, but they don’t make for more square chin shapes. They just make the chin wider with no obvious squareness. Your current result is very reflective of the implant’s design shortcomings. I have learned by extensive custom chin and jawline implant designs that to create a truly square chin shape the implant must have an exaggerated square chin shape with profoundly square corners but also not excessive width in so doing. A 33mm to 35mm wide distinctly square chin implant design works better in that regard in my experience. (see attached) Perhaps one day an improved square chin implant will be available as off-the-shelf item but until then custom designing it is the way to go.
A: As you have pointed out I have never found the standard square chin implants (Terino style 1 and 2) to be very aesthetically satisfying. They have rounded corners, which are wider than the rounded anatomic chin implant styles, but they don’t make for more square chin shapes. They just make the chin wider with no obvious squareness. Your current result is very reflective of the implant’s design shortcomings. I have learned by extensive custom chin and jawline implant designs that to create a truly square chin shape the implant must have an exaggerated square chin shape with profoundly square corners but also not excessive width in so doing. A 33mm to 35mm wide distinctly square chin implant design works better in that regard in my experience. (see attached) Perhaps one day an improved square chin implant will be available as off-the-shelf item but until then custom designing it is the way to go.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How is it possible to to lengthen the clavicles without expanding the upper ribcage? How does postoperative functionality and biomechanics compare to people with naturally long clavicles?
A: When the clavicles are lengthened the ribcage is unaffected. The ribs are connected to the spine and the sternum and are not influenced by changes in the clavicle which lies above it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a couple of questions regarding correction of Plagiocephaly.
1. What deformities are able/not able to be corrected.
2. How often are people unhappy with the corrections that have been made
3. What is a general cost estimate for a Custom skull implant, along with reduction of the forehead if there is any way you could estimate.
4. Is there any way that the bottom part of the back of the skull could be augmented? The flat side of the back of my head seems to bulge out near my neck more than the other side.
Thank you very much!
A: In answer to your plagiocephaly questions:
1) All aspects of the skull affected by plagiocephaly can be treated, whether it is by augmentation or bone reduction.
2) Patients may desire further improvements but no one has ever been unhappy with the result in my experience orawareness.
3) My assistant Camille will answer the cost question.
4) The bottom part of the back of the skull can be augmented.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, what are the of outer limits of iliac implants projection from the iliac? how wide, long and thick can they be? (excuse me if my language is imprecise), what is the maximum longitudinal/axal/transverse length an implant can go from the iliac crest, and what is the maximum sagittal/ longitudinal width one can make a implant? what is the maximum thickness of the implant? having been disappointed in the results from silicone hip augmentation, i want to make sure that this implant is more grounded and realistic on the actual results rather than my hopes. as i said, i am tall an weigh close to 200lbs with a rectangle body type. although i have had my lower ribs removed for eventual corset training. Unfortunately, I’ve had to learn the hard (and expensive) way that implants that might be dramatic or extreme on a petite or average female body, barely register on me. as i think I mentioned, my current silicone implants were the largest pre designed ones that the surgeon i went to offered, and would look exaggerated on petite/average bodies, but fell far short of what i’d hope on my body. i have always aimed for something close to a ‘coke bottle/hourglass if not bottom heavy pear shape. so this extra information will help me decide if this is worth pursuing iliac implants, larger custom silicone implants, or a combination.
Thank you for your help in advance.
A: I think when you look at your height and weight I am not surprised that just about every ‘standard’ implant used will make a negligible difference, particularly given your goals. The issues with hip implants, and I wlll classify standard hip implants (below the iliac crest) and iliac crest implants (at the actual iliac crest) as hip implants, is that the larger they go a significant increase in complications will occur. The hip area is particularly unique and challenging area to augment for a variety of reasons. Beyond 30mm of iliac crest augmentation and above 400cc hip implant volumes are really uncharted waters so to speak where few patients have ever gone. Uncharted waters does not mean one should never sail in them but everyone needs to be aware that lessons are often learned by doing so and I would prefer not to learn those lessons on actual patients if it can be avoided.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I currently have fillers in my chin and jawline. I am considering geting a permanent custom chin/jawline implant but I was wondering how long I would need to wait since my last treatment of fillers before i am eligible for implant, or, if there is a certain protocol (dissolving, waiting a certain period of time, etc.) Thank you!
A: Good question. As a general rule I usually do not ask patients to dissolve their fillers before custom facial implant surgery. They do not interfere with the implant design process nor the surgical placement of the implant. Whatever fillers are left at the time of surgery, the trauma of surgery will quickly dissolve the remaining fillers present.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, With the addition of a peek implant to only the forehead to increase bone thickness and prominence of the forehead, will it automatically cause the top of the head to also look slightly fuller? This is because I imagine that the skin would have to stretched over an extra area over the newly inserted peek implant so the top of the head/overall head shape may look slightly different when stitching back the incision after inserting the new forehead implant?
Many thanks for your help.
A: The front part of the top of the head will have to increase as the footprint of the implant has to extend back further to blend in and have a smooth and natural contour. The material used is irrelevant, the forehead implant design principle remains the same.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, 1. I am an Asian, but can you make my eyes go deep like Westerners with orbital box osteotomy?
2. Is this surgery as dangerous as the Lefort3 surgery?
3. If it is possible to operate deeper, I wonder if the size of the eyes will decrease or increase .
A: The only effective and safe way to make the eyes deeper is periorbital augmentation. Orbital box osteotomies can move the eye horizontally or vertically but can not make the eye look deeper.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I’m interested in a genioplasty revision. To give you context, I had a genioplasty a couple of years ago where my chin was moved forward 8mm and down 3mm, about 8 months later I went in for a revision to have it reversed. The surgeon used the burring method, it’s been over a year and my chin looks bulky, flat and vertically longer than my original chin. I don’t think he did a good job, it could be excess soft tissue or maybe he didn’t reduce the bone vertically enough. This situation has been distressing to say the least.
I think a 4 to 5mm vertical reduction will make it fit my face shape better more closely resemble my original chin. I know you are one of the few experts in this area and I would really appreciate his input and wish he can help with this.
A: Trying to reverse a sliding genioplasty is not best done by burring as, while that reduces some horizontal bone projection, it will create a definite soft tissue chin pad redundancy. Not to mention that a burring technique done intraorally can not reduce the vertical height of the chin.
To now reduce the bony height of the chin, which will further magnify the soft tissue redundancy, it may be best to take a submental approach so both vertical bone height and the soft tissue chin pad redundancy can be simultaneously addressed.
But to provide a more informed recommendation reviewing the CBCT scan would be necessary.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I don’t have syndrome, but I’m stressed because my mid-eye area is very flat. I know that Lefort3 surgery is very dangerous, but I wonder if Lefort2 is also a very dangerous operation to receive for cosmetic purposes.I know there is a prosthesis in the mid-face, but I really want to have a surgery for Lefort2.
A: No form of a LeFort advancement is ‘dangerous’ but it is a major midface surgery that has its own issues/tradeoffs. Whether one is a candidate for a Lefort II procedure depends on their current occlusal relationship and whether a simultaneous lower jaw advancement needs to be performed with it to keep a good occlusion intact.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to extend the collarbone 3 or 4 times for a total of 12cm or 16cm? I want to get an extension effect of 12cm or more through at least 3 surgeries. Is it possible if there is enough time and rehabilitation?
A: Such a degree of clavicle lengthening (12 to 16cms) is not possible no matter how many times it is done. The tight shoulder girdle and scapula is the limiting factor that will prevent the clavicle from being lengthened that far.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am looking to get a consultation on a BBL – reconstructive surgery. Reaching out to you based on your previous experience in handling similar surgery (Plastic Surgery Case Study – Buttock Reconstruction with Dermal-Fat Grafts).
To give more context, I had a childhood trauma which resulted in a deep scar on one side of my butt. I would like to schedule an appointment with the doctor to discuss the options (regular injected fat vs dermal fat graft vs implant / other options) and the doctor’s availability. I’m planning to get it done as early as possible.
A: Thank you for your inquiry and sending your picture. While I can see your scar I can not tell how contracted or tightly adherent it is. That aspect of the scar is crucial as that determines whether just proceeding with fat injections (minimally adherent) or whether a dermal-fat graft is needed. (moderately to tightly adherent) Because the injury occurred in childhood it is likely the latter in my experience. If so I would do the scar release/dermal fat graft first followed by a BBL after.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am reaching out as I would like to investigate the possibility of getting a forehead implant and a jaw and chin implant.
My main concern is the shape of my forehead, which gives me a bit of an egg-shaped look and ages me somewhat. There are 4 main problems I have identified:
1) the angle at which my forehead slopes is too great, giving me a neanderthal look
2) From the side, the curvature of the front half of my skull exacerbates the egg-shaped look (I think an implant would need to start some way up my skull to compensate, and give my skull a more flat, square look from the side)
3) My forehead has little support at my temples, again contributing to the egg-shaped look, giving a hollow and aged appearance, and this is in contrast to my cheeks and jaw which extend further out
4) the indentations in the middle of my forehead and above my eyebrows really trouble me, especially in photos. I believe some improvement could be achieved with botox to atrophy the brow muscles, and some filler to smooth out the indentations, but because of the 3 above issues identified, I think an implant is the most sensible option! 🙂
Thank you so much for your time. I look forward to hearing from you.
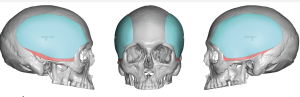
A: Thank you for your inquiry and sending your pictures. You are spot on in identifying in that the correction of your forehead slope/shape extends well beyond the forehead itself. It involves the need to reach up and cover the top of the skull as well as wrap around the sides (temples) to get a smooth uniform effect. (see attached imaging) This is reflective of the anatomy of the overall skull which is a collection of 5 convex surfaces. Most skull augmentations have to cover at least 3 of them to get a uniform and natural looking effect. In you such a forehead augmentation must cover 3.5 surfaces (forehead, temples and part of the top of the skull)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I was just curious if a silicone implant place could success push out a moderate labiomental fold. I read in one of your studies that cadaver material such as gortex could be used but would make only a modest difference. For someone who wants the fold more straight and pushed out, could a thicker implant such as a customized silicone implant work better?
A: No form of underlying bone augmentation will push out a deeper labiomental fold as the fold is reflective of the origin of the mentalis muscle to the bone. Improving the depth of the labioimental fold requires soft tissue augmentation. (right under the skin but above the muscle) Whether that should be done by fat injections, the intraoral placement of a dermal-fat graft or some form of a subcutaneous implant can be debated. Bur regardless of how it is done the result you have imaged (a completely eradicated fold depth) is not possible. Halfway between your original fold depth and what you have imaged is a more realistic outcome.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I lack confidence because of my thin and narrow face, I think I look feminine which is not so good. I have a long bottom jaw which is steep. Can mewing work or should I get surgery for implants?
A: The only predictable and sustained method for jaw augmentation is implants. Mewing can not produce the type of jaw augmentation changes that implants can and, once in place, would require no work to maintain the result.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I need some information about hollowness between eye and brow. Is it possible to use bone graft to fill the hollowness and lowering the supraorbital area. What do you prefer to use on that case. But remember please, only permanent result.
Is it better using implant or bone grafts. Usually plastic surgeons use filler or fat graft but i do not like temporary result.
A: As a general statement while either bone graft or implants can be used to augment/lower the supraorbital rim/brows, custom implants are preferred because they will have a predictable preoperative determined shape, can be inserted through much smaller incisions and will have an assured smoothness. The same can not be said when it comes to bone grafts….not to mention the need for a harvest site.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a small round bony protrusion on the middle of my forehead paired with a browridge. I was wondering if it would be technically possible to shave this bone and add this excess of bone to the browridge ? Thank you very much for your time.
A:While the mid-forehead bony protrusion can be removed and added (recycled) to your brow ridge, such bone grafts will add very little volume and will likely undergo 100% resorption very quickly in the early postoperative period. So the question is not whether such bone transfer can be done but that will be ineffective both in volume addition and in retention.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted your medical opinion on the potential approaches to rib removal surgery. Regarding the rib removal, we discussed the big impact of having the 10, 11, and 12 ribs resected. I would like to hear your thoughts on the following and I have included images (attached) to aid in clarification of what I am trying to ask.
1.- Latissmus muscle resection
During my consultation you mentioned you normally resects the lower part of the latissmus muscle (I show on the image as red). Would it be possible to remove a longer segment for a greater trunk width reduction? I have a broad back and would be interested in this possibility but wanted to hear his thoughts on risks or considerations (reduced strenght, reach, etc).
2.- Rib Resection
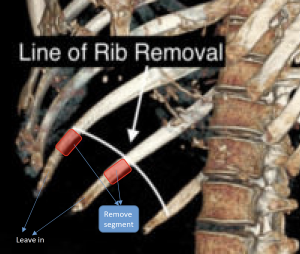 Would there be any benefit or risk to instead of doing the traditional rib resection procedure only removing a segment and leaving the remaining “frontal/tip” part of the rib floating? Would this give some protection or would this reduce the waist reduction effect? Would this turn into bigger risks with puncturing organs, rib flail, etc?
Would there be any benefit or risk to instead of doing the traditional rib resection procedure only removing a segment and leaving the remaining “frontal/tip” part of the rib floating? Would this give some protection or would this reduce the waist reduction effect? Would this turn into bigger risks with puncturing organs, rib flail, etc?
A: In answer to your two excellent waistline narrowing questions:
1) It would produce even better results to take a longer strip of latissimus dorsi muscle but the limited flank incisions used for rib removal surgery only permit the wedge of muscle to be taken to be so big/long. A vertical incision on the side of the waistline would permit a much longer width of the muscle to be removed but the aesthetic tradeoff of the scar may be questionable.
2) Your question is whether removing just a central section of the rib and allowing the remaining outer portion to float would produce a similar result as removing the entire outer half of the rib is a good one….and one I have often thought about doing. (rib osteotomy vs rib removal) I suspect if one employed short term corseting to help shape the waistline that it may have similar results as the bony lateral support of the waistline is reduced.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have scheduled for paranasal implant surgery in September. Now I would like to ask you a few more questions about it:
- Do you think it will be advisable to stay in Carmel for 1 or 2 weeks after the surgery in case some complications may occur?
- Can I eat normally the days following the surgery or are the any restrictions?
- Is it possible to have another surgery done (some months) after the paranasal implantation? I am thinking about a facelift in early spring of next year. From your medical point of view, would this be a problem after the paranasal implantation? Will the implants affect the feasibility of a subsequent face lifting in any aspect? Is the planned point of time 4-5 months after the paranasal surgery ok or should I wait longer? Would it be even better to have the face lifting done prior to the paranasal surgery?
A: In answer to your paranasal implant surgery questions:
1) One to two weeks stay after surgery is not necessary. Infectious complications, rare as they may be for the midface, won’t occur until 3 to 6 weeks after the surgery.
2) I would be careful about biting off food for a few weeks with the high vestibular incision. This is easily bypassed by using utensils to replace what the front teeth normally do.
3) You could have any form of facelift surgery within weeks or months after the paranasal augmentation. Such central midface implants have no impact on mid- or lateral facelift surgery, whether done before or after.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I want a wider head shape with a temple implant. What shape should the implant be?
 A: Thank you for your inquiry and sending your pictures. Because it really involves the side of the entire head a wrap around or extended temporal implant style (head widening implant) is needed to create an harmonious change from the side of the forehead back to the posterior temporal region. It doesn’t have to be very thick (5mm max most likely in the center) but it is the footprint of the implant that is most important in achieving the desired effect. You also don’t want to overdo the width of the implant to keep in balance with your thinner face and what appears to be a leaner body shape as well.
A: Thank you for your inquiry and sending your pictures. Because it really involves the side of the entire head a wrap around or extended temporal implant style (head widening implant) is needed to create an harmonious change from the side of the forehead back to the posterior temporal region. It doesn’t have to be very thick (5mm max most likely in the center) but it is the footprint of the implant that is most important in achieving the desired effect. You also don’t want to overdo the width of the implant to keep in balance with your thinner face and what appears to be a leaner body shape as well.
Dr. Barry Eppley
Indianapolis, Indiana