Your Questions
Your Questions
Q: Dr. Eppley, Last year I underwent surgery to improve the mandibular contour through personalized PEEK implants in the chin and jaw. About 3 months after the operation, I had an infection plus a posterior lump on my left side. The doctor drained it, but soon after the abscess turned into a fistula that oozes pus continuously, and it’s been like that for several months. As a consequence of this, the maxillofacial surgeon now proposes to remove the implants as the infection plus abscess and fistula came out as a result of, according to his criteria, a body rejection of the PEEK implants.
My questions are:
What has happened to me is due to a rejection (as the doctor assures) or to a potential contamination of the implants before the intervention?
Can you provide me with some hypotheses about why the infection plus posterior abscess and fistula have appeared?
Can I go through the same surgery after the current implants have been removed and mouth healed, or there’s any reason/something preventing me to do it?
Can this happen to me again or is it unlikely?
Thanks in advance for your help.
A: Throw out the concept of ‘rejection’ of the implant as that is not a biologically accurate explanation…this is an infection….a known risk of any implant surgery and the risks are higher when the implant is introduced through the mouth which is not sterile and can not really be made to be so at the time of surgery.
Implant Infections fool patients because they occur much later than patients are aware…anywhere from 3 weeks to 3 months after the surgery. (most do occur by 6 weeks) When they occur the implant fate is largely sealed due to the development of biofilm on the implant which can not be eradicated by antibiotics alone. Antiubiotics may suppress it for a period of time but can not usually cure it. Removal of the implant is the definitive cure. Implant replacement can be done 6 to 12 weeks later. The risk of implant infection is the same each time the surgery is done. The key question is always what is going to be done differently the next time to try and prevent it from occurring again.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in the procedure of Rib removal. Can you please provide me more information. I want to know if the ribs are going to be removal or just break them and leave it inside the body. I’m a little confused about that part.
A: Thank you for your inquiry and sending your pictures. There are two methods of waistline narrowing by lower ribcage manipulation, removal vs fracture. I most commonly perform rib removal for waistline narrowing which also includes flank liposuction and muscle trimming…which provides the most comprehensive approach to the inward movement of the waistline. Rib fracture is as the name implies where the ribs are cut and left in place and relies heavily on postoperative corseting to achieve some inward waistline movement. The rib fracture method does not produce as much of a result as rib removal but offers a less invasive surgery and a quicker recovery.
Barry Eppley, M.D., D.M.D.
World Renowned Plastic Surgeon
Q: Dr. Eppley, Im interested in the procedure of Rib removal. Can you please provide me more information. I want to know if the ribs are going to be removal or just break them and leave it inside the body. I’m a little confused about that part.
 A: Thank you for your inquiry and sending your pictures. There are two methods of waistline narrowing by lower ribcage manipulation, removal vs fracture. I most commonly perform rib removal for waistline narrowing which also includes flank liposuction and muscle trimming…which provides the most comprehensive approach to the inward movement of the waistline. Rib fracture is as the same implies where the ribs are cut and left in place and relies heavily on postoperative corseting to achieve some inward waistline movement. The rib fracture method does not produce as much of a result as rib removal but offers a less invasive surgery and a quicker recovery.
A: Thank you for your inquiry and sending your pictures. There are two methods of waistline narrowing by lower ribcage manipulation, removal vs fracture. I most commonly perform rib removal for waistline narrowing which also includes flank liposuction and muscle trimming…which provides the most comprehensive approach to the inward movement of the waistline. Rib fracture is as the same implies where the ribs are cut and left in place and relies heavily on postoperative corseting to achieve some inward waistline movement. The rib fracture method does not produce as much of a result as rib removal but offers a less invasive surgery and a quicker recovery.
Barry Eppley, M.D., D.M.D.
World Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to have a small revision genioplasty as my chin was moved too far forward and down, but would not like titanium plates and screws to be in my body. I read that you did a paper on using reabsorbable polylactic-polyglycolic acid plates and screws, claiming they were an effective alternative. Would this be possible for a 2mm reduction genioplasty? I would be willing to have a consulation and procedure with you if possible. Please advise on the reabsorbable plates and screws in particular.
 A: Thank you for your inquiry. I believe what you are specifically desiring is an intraoral secondary genioplasty where the titanium plate and screws are removed, an osteotomy is done to set the chin back by 2mms and the chin bone fixed into position by 2.5mm resorbable lag screws. (see attached) That can certainly be done.
A: Thank you for your inquiry. I believe what you are specifically desiring is an intraoral secondary genioplasty where the titanium plate and screws are removed, an osteotomy is done to set the chin back by 2mms and the chin bone fixed into position by 2.5mm resorbable lag screws. (see attached) That can certainly be done.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have a question about midface (nasomaxillary) projection. My nose(practically entire mid-face) from profile looks quite flat and my cheek line” from profile is almost vertical. I would prefer to have a nose that projects more and a more sloped cheek line. In the book “Aesthetic Surgery of the Craniofacial Skeleton: An Atlas” I read about some osteotomies that advance fragment of nasomaxillary complex and advance it forward and counterclockwise (but I don’t know if such procedures are performed on a regular basis.
Traditional bimaxillary surgery won’t bring the nose forward so its not really an option. Below I attach pics of my nose, what I meant by cheek line and desired midfacial side profile.
Thank you very much for answer.
A: Thank you for your inquiry and sending your picture and detailing your concerns and objectives. It is esay to get caught up in facial osteotomy designs on drawings and assuming that is the best way to address their facial concerns. In reality these osteotomies have their place but when it comes to increasing the projection of the nose on an otherwise flatter midface this would not be an effective method to do so. (nasomaxillary augmentation)
First you have to define exactly by what you mean by ‘increased nasal projection’. This could entail one of two meanings…increase the projection/fullness of the nasal base or improving the projection of the dorso-columellar line of the external nose. I am going to assume you mean the former since you have described your own lack of midface projection and have been looking at osteotomy approaches to improving it. In that regard it is far more effective and surgically less complicated to adding to the flatter midface, specifically around the bony pyriform aperture around the base of the nose. This onlay augmentation can be done by bone/cartilage grafts, bone cements and custom implant designs. There are advantages and disadvantages to all of these onlay midface augmentation approaches which requires a more detailed discussion.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! I have two questions: one, how much does rib shaving cost (or could you give me a start-up estimate)? Two, is it possible to shave down the width of a ribcage? Mine is terribly wide and it gives the illusion of a male shape. This is NOT what I want. I’m also a bit short, which makes it worse! I’d love more of a rectangular shape. Almost adolescent in nature. Thank you!!
A:Rib removal surgery is for specific areas of reductions around the ribcage like the waistline or the subcostal margin. It can not be done for an overall ribcage width reduction as that involves too many ribs to try and reduce. It would not be effective for that aesthetic ribcage concern.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi, Ive asked questions on here before but I had another one that is a big factor on wether i would like to get work done.
When getting multiple procedures done (plagiocephaly in my case), does it cost the same as all of the procedures separately or is there a bit of a discount since it’s being done all together? I would also love to know how much past full plagiocephaly corrections have costed, as price is a huge factor.
Thank you!
A: The economic benefits of combining procedures comes from the reduction of OR and anesthesia costs. When doing procedures separately there is time to get the patient ready in surgery and time to apply dressings and wake them up which is part of the surgical cost. When combining procedures these ‘startup and closing down’ time/costs are reduced and become one rather than multiple additive units when procedures are done separately.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi. Does you charge same price for shoulder widening even when you only operates on a single shoulder to fix asymmetry? Also how much of lengthening can be done?
A: Thank you for your inquiry. When only one clavicle is being operated on the cost would obviously be less than bilateral clavicle surgery due to a shorter operative time and less hardware used. How much clavicle lengthening that can be achieved depends primarily on the reason for the shoulder asymmetry. Is it a congenital shoulder asymmetry or a traumatic one induced by a fractured clavicle? The next question is how much clavicle lengthening is needed? (based on x-ray measurements) The answer to these questions is needed to address how much clavicle lengthening can be done…or more pertinently how effective would such surgery be.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Is it possible to extend the collarbone 3 or 4 times for a total of 12cm or 16cm? I want to get an extension effect of 12cm or more through at least 3 surgeries. Is it possible if there is enough time and rehabilitation?
A: Such a degree of clavicle lengthening (12 to 16cms) is not possible no matter how many times it is done. The tight shoulder girdle and scapula is the limiting factor which provides a ‘stop’ as to how much push the extended clavicle can be allowed to go..
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I wanted to get a bit of information on your custom wrap around jaw implants to reshape my jaw line. I had recently had a Bilateral Sagittal Split Osteotomy and Sliding Genioplasty to correct a Class-II Malocclusion. I am currently unhappy with the shape and position of my lower jaw. As it stands I have a jaw that has downward growth; it has a high gonial angle, lacks bi-gonial width, short ramus length, and my chin is a bit recessed. My Maxillofacial surgeon recommended that I find a surgeon that has extensive experience working on reshaping male patient’s jaws. I had spoken to a few plastic surgeons but what caught my attention about your practice was an article you wrote titled “Plastic Surgery Case Study – Custom Jawline Implant Design for the High Gonial/Mandibular Plane Angle Patient”. In this article you went into detail about your procedure to bring a male patient who had a high gonial angle of 150 degrees down to 130 and the importance of understanding the relationship between lowering the gonial angle and the masseter muscle in surgery.
I wanted to know if you have any experience working on patient’s who have had orthognathic surgery and if a custom wrap around jaw implant could help me get a more ideal male jaw shape.
A: Thank you for your inquiry. Approximately 20% of all custom jaw angle and custom jawline implant patients have had prior orthognathic surgery for the very reason you are experiencing. Orthognathic surgery serves a very valuable role in facial bone surgery but it is primarily affects the sagittal dimension of the face and is very limited dimensionally in what it can change thereafter. This is why it is not rare to see patients who have had single or double jaw surgery seek to use the jaw surgery as a foundation on which to create enhanced 3D features of their facial bones.
I would refer you to www.eppleycustomfacialimplants.com to look at some of the many jaw implant designs I have done in such patients.
Dr. Barry Eppley
Indianapolis, Indiana
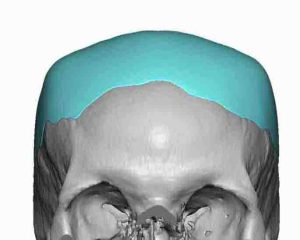
Q: Dr. Eppley, Can my skull be cut down 1 to 1.5 inches from back and my face become normal?
A: How much skull reduction can be done from the back requires an x-ray to evaluate the thickness of the bone. But even at the thickest 1.5 inches of skull reduction can never be done as no one’s skull is ever that thick.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I would like to inquire about options that are available to fix the dent in my son’s head which is the result of a head injury and subsequent cranioplasty surgery. I am also interested in having his scar removed if possible. Please let me know if this is something you can help with?
A: Thank you for your inquiry and sending your son’s pictures. I am going to assume that the prior cranioplasty surgery was a craniotomy bone flap which has subsequently sunken in as it healed. (meaning there is a stable base of bone albeit with less than the desired contour) To achieve both objectives, skull contour restoration and reduction of the scalp scars, requires a combination of scalp expansion (first stage scalp expander placement) and 2nd stage onlay skull reconstruction/augmentation to build out the skull contour. Two stages are necessary as expanding the skull contour without more scalp tissue to cover it will not result in less of a scar appearance. Conversely excising the scars can only be done at the same time if the skull contour is only improved slightly.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have prominent bulging temporal arteries bilaterally. My regular plastic surgeon is against arterial ligation in the area of my temples, out of fear that once one artery is ligated, another will pop up in its place, and thus conveyed to me that there is no surgical solution to bulging temporal arteries (the squiggly pulsing arteries on either temple, they have been confirmed to be arterial.) id love to schedule a consult with one of you surgeons. I am in California so I would need to meet virtually or over the telephone, but I would gladly make the trip to your facility if it is determined that there is a probability of success in treating this issue. It is very difficult to find a surgeon to perform surgery on this area. Thank you!
A:In my extensive experience with temporal artery ligation surgery I have never seen other new vessels appear after such ligation surgery. So your plastic surgeon’s theory (and that is what it is when the surgeon has never actually performed the procedure) is unfounded. This is undoubtably because the ligations are done at multiple levels along the course of the artery. The actual risk of the surgery is recurrence along the existing arterial pathway, not the appearance of new vessels. But even recurrence of any portion of the artery is very uncommon, again due to the multi-level ligation approach.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, About temporal reduction surgery. I checked some images on your website about the temporal reduction and saw that the ears get extremely bent for 180 degrees during the surgery. This could be a big problem because I had both ears set back a couple of times and especially the left ear took 6 surgeries until it was more or less OK and closer to the head. I’m afraid that this method could tear something in the ear apart so that they protrude again. Could you give me some more information about this please.
A: That is an understandable concern but not on in which has occurred even in patients with prior otoplasties. That being said one way to limit that concern is to move the incision a bit away from the depth of the postauricular sulcus out more behind the shadow of the helical rim.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have been interested in rib/waist size reduction for most of my life. From the moment I was born, I had large ribs.
That being said, the concept of rib removal has always felt terrifying and littered with too many negative side effects. I’ve known some people that have had it and they have mentioned that they have lost the ability to do some of their basic lifestyle activities. Cycling, weightlifting, etc. Bending in specific ways.
It has always boggled my mind that someone has never thought of a way to do this by reshaping the ribcage. I always thought dentists and orthodontists do incredible things with teeth. Increasing jaw widths, moving teeth, etc.
After continually searching, I finally found a procedure pioneered by a process of Waist Narrowing without Removal of Ribs. I was curious if you were familiar at all with this procedure and/or if you or anyone else in the United States had began its implementation?
A: Thank you for your inquiry. I have done hundreds of rib removals and have never see the complications/lifestyle limitations you have described.
But that issue aside I am very familiar with the rib fracture technique which is simply a scaled down version of the rib removal procedure, limited to ribs 11 ands 12 and relies heavily on postoperative corseting. Whether it is as effective as the more complete approach to rib removal surgery I can not say but my feeling is that it is for the patient who is more comfortable with a less invasive procedure and is willing to commit to 2 to 3 months of corset use.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am German Male and 2 years ago I underwent a chin wing surgery for 5mm forward movement. I am now looking to reset/reverse this procedure. I am aware that a full reversal chin wing, brings various risks with it. Particularly, the resuspension of the mentalis muscle seems to be a challenge often articulated, when conducting research on the internet.
1. Judging by your cases and personal experience, how likely is it that a patient will need additional surgery for a mentalis resuspension after a full reversal of a chin procedure (genio/cw).
2. As I live in Germany, I am looking for a qualified surgeon in Germany. Do you have any personal recommendations?
A: In answer to your chin wing reversal questions:
1) Mentalis muscle resuspension would be done as part of the chin wing reversal as prevention is better than finding out later it is needed.
2) and 3) I do not have any familiarity with German surgeons so I can not be helpful in that regard. Although it would seem most logical to have the surgeon who performed the procedure undergo the reversal??
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I have just discovered your clinic, I am delighted because I have long wondered if it is possible to have implants on the forehead as well as the skull, in order to have the upper face wider and rounder, as women with a big forehead often say are more attractive! That’s why I come to you because I’m interested in this intervention. I would like to have the same surgery that you posted on your Instagram page on January 26, 2022.
A: Custom forehead implants is a procedure that I commonly do. All. forehead implants have to have some amount of extension that extends onto the top of the skull to blend into bone in as smooth fashion. If you send some pictures of your forehead I can so some predictive imaging on potential forehead augmentation changes.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had buccal fat reduction about a year ago and am less than happy with the results, I am wondering if there’s a permanent procedure you can do to restore some of the fat that was taken out. Please let me know, thank you!
A: Reversal of buccal lipectomies can be done two permanent methods, buccal space fat injections done externally or the direct intraoral placement of a dermal-fat graft back into the buccal space. Each approach has is advantages and disadvantages. Fat injections are less invasive, acquire the injectate by liposuction harvest but like all fat injections their volume retention is unpredictable. A dermal fat graft is the true buccal lipectomy reversal is that a piece of fat is put back directly by which it was removed with a high volume retention rate but it does require an excisional harvest from somewhere on the body.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello! 6 months ago i have a kick direct in to my forehead glabellar bone, and even now i have some times pain in the hole inward in my forehead. Please, I need help with that, i am from Romania and here the doctors recommend me lifting mods for be cheapest. But the pain, and even blocked sinuses some times, are knockin me down most when i try to sleep, or do sport, or i go outside when are much than 77 degrees Fahrenheit. More than that the hole also make me feel uncomfortable sometimes about esthetically. I write this message with the hope can you help me, after i see all the results of you work on this website page. Thanks for the time accorded to read.
A:If I understand your situation correctly you probably have an inwardly displaced fracture of your frontal sinuses (brow bones) creating a depressed dent in the glabellar region as well as a sinus blockage. I would need to see some pictures of your forehead to confirm. But the treatment would be frontal sinus fracture repair, most likely using a cranial bone graft.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello. I’m 28 years old. I already got testicular implant surgery 1 year ago, and planning to replace it with bigger implants. But there were no existing implants bigger than 40cc. Do you make those custom implants with 3D implants? Or do you carve it?
A: All testicle implants over 5cms are custom made by a 3D design process. I have made and placed testicle implants up to 7.5cm with 110cc volume.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, s it possible to change the cheekbone’s shape/cheek hollowing (to a straighter, higher set one)? I‘ve been reading a lot about “the high cheekbone” look, custom infraorbital malar implants and zygoma reduction osteotomies, and there’s something I haven’t seen mentioned.
Most people getting zygoma reduction are Asians (and don’t have the high cheekbone look in mind) and most people getting custom infraorbital-malar implants have very flat cheekbones to begin with.
My question is:
Can someone that already has hollow cheeks change their shape? Let’s say, someone with cheekbones like Jon Kortajarena or this morphed face (prominent, with a curved inwards shape) wants to obtain more straight, vertical cheekbones, like Henry Cavill or this other morphed face. Is that possible to achieve? What procedures would be necessary to do so if possible?
I’ve attached you photos of people with the lower set, curved cheekbones (Kortajarena, Morphed face 1) and the higher set, more vertical ones (Henry Cavill, Morphed face 2).
Would love to hear your thoughts about this.
A :As long as the need is augmentation to achieve the more ideal cheekbone shape then anything is possible with 3D designed implants. If a bony reductive change is required to achieve that shape then the type of change achievable is more limited.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, My eyes are so asymmetrical they stick out like a sour thumb in every picture and in certain lighting. I really need to do something about this but I don’t even know where to begin because every doctor says something different. It’s definitely orbital asymmetry. What can be done about this?
A:Thank you for your inquiry and sending all of your pictures. What you have is a classic vertical orbital dysfopia (VOD) probably in the 3mm range. In VOD the eyeball and all structures around it are positioned lower than the other side. While the eyeball can be raised up the correction is not quite that aesthetically simple as all the surrounding structures (eyebrow, eyelids and cheek) are made for where the eye is now. So just moving the eyeball alone will actually make the asymmetries worse.
There are two fundamental approaches to VOD…complete correction or camouflage. Each approach has its advantages and disadvantages. In complete correction all the structures are treated. (raised) In camouflage the eyeball is left alone and the most obvious causes of the surrounding asymmetry are treated. (e.g., eyebrow and eye corner lifts) See attached imaging to show the differences.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I’ve been reading about hip augmentations specifically iliac crest implants, and the silicones ones you’ve been offering. My question is, do you think the South Korean version (the titanium implant) is even safe the way you would have to put the screws in incase of removal? Also, I was wondering if you’ve yet had any patients with your silicone version, as I am highly interested and how safe those are for removal, as well as price ranges. I check for updates almost every day. Thank you!!
A: Thank you for your inquiry and sending your pictures of which I can appreciate your interest in iliac crest implants. In answer to your iliac crest implant questions:
1) Titanium iliac crest implants are safe but you are referring to how easy they would be to remove if necessary. (reversibility) They can still be removed as the screws merely need to be backed out to do so. There is not that much tissue adhesion to metal other than any perforations in the implant’s surface.
2) Silicone iliac crest implants, which have their own appeal and still require screw fixation, awaits the first patient for implantation.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I had a genioplasty two weeks ago and I hate the results. I’m a 23yo female and my chin now looks square and strong. I wanted to know how long I should wait to get it reversed since I don’t want my soft tissues to sag if I wait too long. I would like to schedule a virtual appointment with you to talk about it. The after pictures are the ones with the white shirt and the rest are the before. Thank you
A: I am sorry to hear of your initial dissatisfaction with the early results of your sliding genioplasty procedure. While it is true that early swelling can make one think their result is excessive when I get contacted by a patient who hates their early result they do not change their minds later about it when the swelling subsides. The two questions that matter then is 1) when should the revisional surgery be done and 2) it is total or subtotal genioplasty reversal. I did not see any before pictures in your inquiry and I do not know if you had preoperative computer imaging so you could look at various options of chin augmentation change but there was a reason you had the initial surgery so usually it a subtotal as opposed to a total reversal in most cases. I would need to see the preop pictures and do imaging to help you make that decision. In regards to timing, if you are absolutely sure this is not the result you were seeking then sooner is better than later.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hello, I am interested in looking into the buccal fat removal procedure. I am looking for a way to make my face less ‘puffy’ and round especially when smiling. I was interested in finding out if this could be an option for what I’m looking to achieve. Thank you!
A: Thank you for your inquiry and sending your pictures. The cheek fullness to which you refer is anterior to the buccal fat pad and thus this procedure would not be effective for you. In addition any form of surgery is geared toward static problems while your primary cheek concerns are dynamic in nature. I(smiling) In other words there is no effective surgery for cheek fullness that primarily appears when one is smiling. Your facial concerns are extremely common but I know of no procedure that I can confidently say will solve it.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I recently had a lip lift which has turned out extremely unflattering, I would like a second opinion, to see what if any procedure can fix it, as I am avoiding being seen and dreading returning to work, I have chosen to not pursue a revision with my surgeon because I believe I may need a corner lift now and I do not believe he does them anyway and I don’t want to risk a second surgery not knowing what to expect and prefer a more experienced surgeon in this field. I know I probably cant have surgery for 6 months but I cant just wait around not knowing when, where, or how I am goin to fix this, and if I have a consult now we can plan a surgery and I can get filler or something in the mean time and then dissolve it before surgery hopefully. My mouth now appears to be very downturned at rest as apposed to horizontal like before my surgery, and my lift seems a lot in the middle and ends before the end of my lip especially on the left side. I look forward to hopefully hearing from you soon thank you for your time.
A: Thank you for your inquiry and sending your pictures. What you have is a classic A frame upper lip deformity from a subnasal lip lift. Such a lip lifting procedure mainly affects the central or cupid’s bow region of the upper lip. Its effects do not extend as far out as the outer lip or mouth corners. This occurs when the absence of significant lateral upper lip vermiliion show is not recognized beforehand. This is where the value of the Q tip lifting test before surgery can be helpful.
That being said you can never reverse a subnasal lip lift as the skin removal is permanent. It is true that there will be some relapse of the lift (up to 20%) within the first six months after the procedure but that never really changes the upper lip vermilion disproportion that is now present. That is treated by lateral vermilion advancements for the outer aspects of the upper lip to create a more harmonious vermilion fullness from one mouth corner to the other. (see attached imaging)
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, How much height can be achieved with skull implants? I’m a model and additional height is never a bad thing. What is the average thickness of a “flat head” implant? What was the largest you’ve done?
A: In answer to your top of the skull augmentation questions:
1) The amount of skull height obtained in the immediate placement of skull implant can be up to 1cm,,,which is how much the scalp can stretch to accommodate it.
2) Larger amounts of skull augmentation can be obtained with a first stage scalp expansion procedure in which I have done as much as 3.5cms of added height.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Hi I want the custom anterior temporal implant design for a head widening effect. My questions are:
1. what are side effects.
2. In case after surgery it is too pain, is it possible to get the injected filler out and back to normal.
A: In answer to your custom temporal implant questions:
1) Such facial implants are not associated with any significant pain so this is not a concern.
2) Any type of facial implant can be removed if so desired although removal due to excessive pain is not a patient problem I have yet encountered.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, I am interested to know if you do 11th and12th rib resection for medical problems as those 2 ribs are pushed inward and up causing pain.I have a case of my left 12th rib syndrome .My 12th rib is not touching my pelvis, its angulated up and inward,being to close to my 11th rib and 11th and 12 crossed toward ends of the ribs.12th rib kind of under 11th, and 11th to curvy and gets stuck under 10th I want to discuss with you rib resection.
A:The typical reason for the medical treatment of ribs #11 and #12 is for ilio-costal syndrome caused by the excessive length of those ribs…which I have done numerous times. Whether that would be effective for those two ribs because they push inward and up I can not say for sure but presumably it would and it requires their length reduction.
Dr. Barry Eppley
Indianapolis, Indiana
Q: Dr. Eppley, Are there skull implants for the side of the skull that could give me a square head shape?
 A: You have correctly surmised that to get a more square head shape you do have to build up the sides along the bony temporal lines. Whether that is done with two separate implants or one implant that thinly crosses the middle can be debated. (see attached) But most likely in your case it would be the former.
A: You have correctly surmised that to get a more square head shape you do have to build up the sides along the bony temporal lines. Whether that is done with two separate implants or one implant that thinly crosses the middle can be debated. (see attached) But most likely in your case it would be the former.
Dr. Barry Eppley
Indianapolis, Indiana