Your Questions
Your Questions
Q: Dr. Eppley, I am a 28 years old and all my life I had a webbed neck and could not find a solution for it. Two years ago, I did physical therapy for a month, it helped a little bit and my neck got slimmer from the sides, but when I stopped, my neck got back to its usual shape. Sometimes my neck is slimmer, some days it is wider. My neck is not so stiff usually. Here are the pictures, I wonder if there are any solutions for fixing it from both sides, and from the profile, the access skin under my chin. I do feel any pain around my neck, and my concern is that I just want to have a normal and slim neck, like everybody. If there is any more information I can provide, please let me know. Best regards
A:You have what I call a mosaic type webbed neck which means it is a moderate webbed neck that is associated with tighter tissues than the full expression of a Turner’s webbed neck where the neck webs are wider with looser/more supple tissues. Improvement in the neck webs is possibloethrough a posterior approach. (see attached imaging) But I would never call it a complete correction or the making of a perfectly normal straight line neck profile. The widened trapezius muscles prevent that complete degree of correction.
Many webbed necks are associated with shorter chins which is a result of the webbed neck. Unless one undergoes a concurrent sliding genioplasty (see attached imaging) the excess tissue under the chin will remain as the submental area is too far away to be affected by the posterior neck tissue movement.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello Have you ever seen case where jaw implants went through skin 8 months after surgery? Intraoral placement, genioplasty before (10 mm forward 3 mm down), chin implant before all of these. After 2 months skin thinning, later scarring, scar burst, red fluid 5 days now yellow fluid no symptoms, sometimes pain when eating hard food. Have my surgeon achieved unique result? I did not find anyone with such problem. Now they want to remove all 3 segments which is disaster. Probably it is because those in the Netherlands prohibited silicone implants. (mine is polyethylene and it was too big)
A:These are not implant-related complications I have ever seen. But it is implants and there is a delicate balance between tolerance and problems which can occur if the implant is too big and/or in the face of chronic infection. The first ominous sign was the skin thinning at 2 months after surgery at which time action would have been prudent as this was a sign that the balance had been tipped unfavorably.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I really would like to see what can be done to address my undereye areas bags, perhaps with an orbital rim implant? And then finally my main concern, the upper third of my face, I don’t hate the brow prominence in and of itself however I would like for some way to ease the transition between brow and forehead. These two problems combined give me a very tired and deficient look from many angles which I hate. Some angles is fine however and when there isn’t a direct lighting the transition is much smoother.
A:You are referring to a combination orbital rim issue with the superior orbital rims (brow bones) too far forward and the infraorbital rims too far back. Thus a combination of brow bone reduction and infraorbital rim augmentation would be the corrective approach. Your face pictures are taken from a far distance so there quality is not great but at least in the side view I have imaged the concept of the potential orbital rim changes.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Is it possible to shorten the nose vertically? Most rhinoplasty results I have seen is because the tip is droopy or long. But in my case the bridge bone looks long and my nostril is lower than my tip. I haven’t seen it done but is it possible to cut/reduce the septal cartilage and reposition the nostril. I hated the way it look long from the front , it looks too far from my eyes.
A:While tip rotation involves making the tip shorter and more uplifted which is a common rhinoplasty change you are referring to a whole nose vertical shortening which is not possible.
.Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Could a surgical hairline advancement be safely preformed via an incision at the hairline in the future if I had a behind the hairline coronal incision already made? If it’s possible without a risk of necrosis or tissue ischemia please let me know how long one would have to wait to have this done. Thank you.
A: No…that would be a very risky procedure for the very reason you have mentioned.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am writing to you because of my facial asymmetry, especially of the eyes, that I am looking to correct. My right eye is positioned lower than the left one and canthal tilt is more negative. Furthermore, my right eye is more hooded and its superolateral orbital ridge sits lower. While my right cheek area lacks volume, on the right side my jaw is more prominent. I was thinking of cheek (right side) and jaw (left side) implants. Concerning my right eye, I was thinking of canthopexy or canthoplasty and brow lift, maybe even orbital floor implant and reduction of the superolateral orbital ridge. What procedures do you think would be most effective in achieving a more symmetric appearance? And what steps would I have to take next to plan surgery with you.
A:Everything you have described is classic for a right vertical orbital dystopia (VOD) including the procedures you have mentioned to address it. An assessment of which VOD and other procedures may be beneficial requires a picture assessment (front view) and a 3D CT face scan which I assume you have not yet had. (you should be able to get that in your country)
Once I have that information I could provide an informed opinion about what the optimal corrective procedures may be. Usually the front view pictures tell us what we need to do and the 3D CT scan provides confirmation of those bony needs as well as serves as the platform on which to build any implants if needed.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had Medpor jaw implants in 2012. In comparing the two sides of my face there is a marked ‘bump’ where the implant is. The goal would be to produce smoother jaw line, to the extent possible (compare with the other side of the face). My fingers show the beginning and end of the implant.
I expect a small reduction in thickness should be enough, but along most of the implant length.There are still screws inside. My doctor said that they can now be removed (during the surgery) The implant on this side feels less regular to my finger. Especially the bottom-outside edge feels sharper and more ‘to the outside’ (this edge is causing the prominence), while the implant on the other side appears more closely following the natural bone.
Very much looking forward to a reply.
A:If I interpret these pictures properly what you are seeking is a width reduction of the implant with a length located between your two fingers along the jawline to which I can say:
1) That cannot be done from the submental incision. It is one thing to put the implant in that way but you are never going to revise that areas of the implant from that approach.
2) This would have to be done from an intraoral approach a direct incision on the bottom edge of the implant to do so..
3) At the location of the most anterior part of the implant lies the exit of the mental nerve from the bone. (marked on your picture as a red vertical line) You would be wise to stay away from that part of the implant to avoid any risk of permanent numbness of the lower lip.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello! Do you see out-of-state patients for rib removal surgery? I have a wide waist/rib cage and flared ribs. I’d like waist reduction, but I live in Omaha, NE. How would the process, operation, and post-op work for out of state patients?
A:Thank you for sending your pictures which show two issues along with your description; flared subcostal ribs and a straight/wide waist line with a lean body frame. While both require rib surgery they are in different locations with different techniques. The flared subcostal ribs are treated by cartilage scoring of ribs 8,9 and 10 with postoperative garments to mold them inward. I feel this technique is better than actual excision due to less visible scarring to do so. Conversely waistline reduction is done by rib removal (11 and 12) with muscle reduction as I find this technique more effectve than the rib fracture method.
Because it is two different surgical locations one has to consider which rib problem is of the greatest priority. While it is technically possible to perform all four rib area surgeries in the same operation I would only do so after evaluating the patient’s recovery issues more carefully.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am wondering if it is possible to reduce the length of the philtrum without increasing the size of the upper lip. I have an 18mm long philtrum combined with already really thick, full lips for a man and I am curious what can be done to shorten the length of it without making my upper lip bigger & longer. could an upper lip reduction be combined with a lip lift to achieve this? Thank you!
A: The simple answer is no if you are referring to the entire thickness of the upper lip. With a subnasal lip lift to shorten the length of the philtrum the same amount of upper lip tissue thickness is being compressed into a shorter external lip length so it will likely get a bit thicker.
If you are referring to the amount of increased fullness that will occur in the vermilion of the upper lip (lower portion) from a subnasal lip lift then the answer is yes. That can be managed by a lip reduction to prevent the vermilion from becoming bigger/fuller. That is not a rare combination for the very concern that you have.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Looking to get custom jaw angle implants, I’ve had ~1ml of filler on both of my jaw angles to increase the frontal width/angularity and it looked great. I saw some of your results and i’m liking a lot of them and would like to possibly get surgery done as soon as possible. I currently reside in Canada, and would like to understand the process. I currently do have filler so i’m assuming that also needs to be dissolved before surgery. What’s the estimated wait time between consultation, implant design/shipping, dissolving filler (I had 1ml done 9 months ago but there’s still a bit of filler left).
A:I assume you have an HA filler which responds well to hyaluronidase injections. I would do that a month before the surgery.
For custom jaw angle implants that is a three month process from receiving your 3D CT scan and the surgery date.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, My chin has been growing with time I feel like it might be due to weight gain as well it shrink and grows sometimes slightly with my weight and sleep I have no idea but it’s squishy and I’m always so insecure of it and I was wondering if you have answers for it or what I can do to get rid of it.
A:With a deep labiomental fold and a bulbous soft tissue chin I can see that there is a likely mismatch between the size of the chin bone and the overlying soft tissue chin pad. That can only be improved by a submental chin pad reduction. The key to how successful that reduction would be depends on how mobile the soft tissue chin pad is…..which would be evident by grabbing it and seeing how much it moves as well as does it pull down when smiling.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to augment forehead to achieve a more full symmetrical look, and eliminate the indented like forehead. And also augment my brow bone area for a more subtle masculine look. Also considering an earlobe reduction.
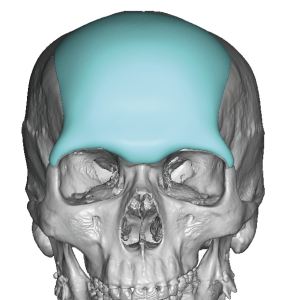
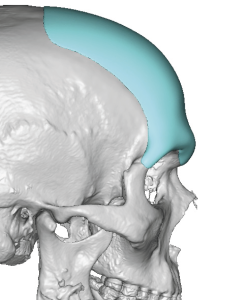 A:You are referring to the need for a custom forehead-brow bone implant which can effective address the total forehead augmentation needs. (see attached imaging) An earlobe reduction can be combined with that procedure during the same surgery.
A:You are referring to the need for a custom forehead-brow bone implant which can effective address the total forehead augmentation needs. (see attached imaging) An earlobe reduction can be combined with that procedure during the same surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I’m interested in learning more about procedures to achieve a more youthful and feminine look, particularly in line with Asian beauty standards. I’m currently exploring my options and would love your professional opinion. Some of my concerns include narrow temples and cheekbones, lack of volume in the lower cheeks and hollows, a small upper lip and long philtrum, a wide mouth, a tired appearance, a sharp protruding nose, and my face appearing too bony. I feel there may be excess fat or bone around my chin and perioral area, creating a square look.
A: To do a proper analysis for your facial reshaping desires I wold need some facial pictures from which I could image what may be possible in changing the shape of your face.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had brow bone reduction a couple years ago via a coronal incision. The surgeon did not reduce the orbital rim on my right side the same as the left (The right side is more prominent). I do not want to go through another coronal approach. Can you fix this through an endoscopic approach or perhaps through a forehead wrinkle? (The difference is difficult to see in pictures but I sent one for you to see what I look like.) Thanks
A: With your deeper horizontal forehead wrinkle lines they would be the incisional approach for your right orbital rim reduction. There is no need for a repeat opening of the coronal scalp incision.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I need forehead surgery as I want a nice large forehead.
A: Based on your picture this is clearly a syndromic forehead shape with a very low hairline and a recessed and flat/concave forehead shape. This needs a significant forehead augmentation which ideally iis done in two stages with a first stage forehead skin expansion so a large forehead implant can be placed secondarily.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, i want my midface to be shorter and closer if possible. My current facial measurement are: brow to chin leght is around 12-13cm, nose is around 5.8cm leght to the tip,face width is around 13.5cm.
My desire are to make the face more striking and stronger bones but also shorter. Also I would like a sunken cheek as shown in the pic but not too much just a little. I will like to know how I would get a low striking eye set.
Thank you
A: i don’t see many of these changes as achievable:
You can’t make the midface shorter or closer together
Stronger and shorter for the face is any oxymoron…you can’t shorten/reduce a face into more strong or defined features. Stronger features come from making them bigger not smaller.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I just had a sliding genioplasty and I have a contracted lip and a step off. How long after the genioplasty do I have to wait until getting the procedure to fix the shortening of the lip?
A: I would wait a full six months to be sure that the initial tightness you feel does not largely resolve.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hi, I am a Canadian citizen that is interested in getting rib remouval surgery, which is not possible in my country. Do you accept international clients for your procedures or can you only perform you cosmetic procedures on American citizens? Thank you kindly for your time.
A: My practice has patients from all over the world with many from Canada.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello, I’ve been interested in custom jaw implants for a long time and actually had non custom angle implants put in years back and one of them popped off when I yawned which eventually led to a hematoma in my cheek. We ended up just removing them to avoid that happening again which has scared me from getting them redone. They were not custom ones and he said the smallest ones were still pretty big for my jaw which. I’ve been a bit scared to have them redone (which if I do I’ll be going to you.) have you ever had anyone’s jaw implants pop off? I’m worried if I go there and return home, and it pops off again that you’ll be so far away. It’s the hematoma in my cheek that scared me. We did leave it in there for around 3-4 days after it popped off until he could redo them so maybe that’s why that happened?
A: Having performed over 1,000 jaw angle and jawline implants, standard and custom and for primary placement and revisions and replacements, I have never seen any implant ‘pop off’ or develop a hematoma after surgery. So what happened exactly to you I do not know. But if popping off of the implant means it moved from its position right after surgery that is completely avoided by using screw fixation. I would go so far as to say that no jaw angle or jawline implant should be placed that is not screwed down.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, hi!! i am a 25 year old female with mild to severe plagiocephaly. my frontal right side of my skull is protruding, along with the occipital right side of my skull being flat. i live in Montana but i am willing to travel to have this part of my skull shaven down (front right) and an implant put in the back right of my scalp. i had a couple of questions regarding the consultation. i see that we can schedule a virtual consultation, but wouldn’t radiographs need to be taken during the consult? i am just worried about traveling to Indiana just to get radiographs, fly back to Montana, then back to Indiana to get the procedure, then back to Montana again. any help would be greatly appreciate as i have been researching this for months and have been wanting this surgery my entire life. thank you so much!!!
A: You are correct n that a 3D Skull CT scan is needed to assess the thickness of the frontal bone to see how much of the forehead protrusion can be reduced as well as it serves as the basis on which the implant is made for correction of the flattened side of the back of the head.
That is a scan you get where you live in which we provide the order for you to get it done at a local imaging center. You only owe here once for the surgery.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I’m a transsexual female and I am wondering if you are able to reduce skull and face width. I have already had a cheekbone reduction so I am not sure if any more can be taken off.
A: I am not sure whether your cheekbone reduction was by shaving osteotomy which would determine whether any more with reduction can be done in t6he midface. The skull and jawline which you did not mention as being yet treated can have width reduced thtrugh temporal muscle and jaw bone reduction. But I would need a front view picture of your head/face to do some imaging to show you how much further craniofacial width reduction can be achieved.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, When considering skull reduction surgery, is the removing include outer cortex of skull, the periosteum and the thin muscle above or just the bony part of the skull ? And if only the bony part , is its possible to remove the muscles fiber that are covering the whole skull in seeking to get more reduction?
A: in skull reduction the entire soft tissues of the scalp are lifted off the bone and it is the bone that is reduced. There are no muscle fibers that attached directly to the bone except at the its ends. (brow bones and nuchal ridge of the occipital bone) The periosteum and all the soft tissues above it are left untouched as all that would do by doing any excision would create a soft tissue contour deformity.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I am not overweight/ but no matter how much weight i lose, i can’t seem to gain a prominent collarbone. I’m looking to change that and am open to suggestions.
A: Having done hundreds of aesthetic clavicle reshaping surgeries I have obsreved there is great variability in the thickness of the soft tissues overlying the bone. Those with prominent clavicle show have a thinner soft tissue cover while those with no clavicle show are buried under a thicker soft tissue cover.. Clavicle show or prominence has very little to do wirth the size of the bone.
That being said I would have little confidence in liposuction to reduce the soft tissue thickness to make the bone appear more prominent. I would have more confidence that enlarging the bone by a sleeve implant would be more effective in that regard.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If I change up the midface implant for just cheek implants that are smaller and more designed like the first design as attached (but still with the brow ridge section), will there be sagging in the cheeks and if yes, where?I’m mainly concerned with the area in between my nose and cheeks.
A: When you reduce the size of an implant, particularly one that ‘hangs off the side of the cliff’ (aka all midface implants) there is always the risk of soft tissue sagging. How likely that is depends on what level of the midface that the implant is reduced. The higher on the midface it is the higher the risk of soft tissue sagging that could occur.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, What will happen when I grow older and my mandible shrinks but the implant will stay the same size. Wouldn’t that be an issue to have custom implant for my whole jawline? Sorry I am ignorant about this. Thanks
A: Your mandible does not shrink with age…unless you lose most or all of your lower teeth.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, If I have a step off and my lower lip is thinner and tight after a recent genioplasty, is this a fault on the doctor’s side? Do I have the right to ask him for a revision or at least a partial refund.
A: These are known risks of the surgery, not signs of negligence or a deviation of the standard of care.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, Hello i have a question about this surgery. I don’t have any injuries in my face but i just want higher cheekbones and i would like to know if this is possible? I know cheek implants might seem like a good option for this but thats not really rhe look i want. I was picturing this as moving or reconstructing the bone so the most peominent part is closer to the eyes and most importantly the cheek below the bone is bigger so the lowest part of the cheekbone is higher. Is this possible?
A:There is no bone moving method (osteotomy) thar can make the cheekbone higher or closer to the eye. Cheekbone osteotomies are lateral inward or outward movements not vertical.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had an Intraoral chin reduction in 2023 and am seeking a second opinion. I’m still unhappy with the aesthetic look of my chin after having it burred down 6mm. It totally changed the appearance from the front and side making it more pointy and projected. I’m not sure if I have excess soft tissue that could be removed or if I need another bone reduction. My chin projects further when I smile rather than resting. After my surgery I now experience sagging skin on my chin that I didn’t have before. From the side it gives off a crescent moon profile which I would hope to be corrected. I would like my chin to be shorter in length as well as less projected. What could be done to give me my desired appearance. (Photos) would this be possible and realistic outcome?
A:The problem with intraoral chin reductions, and is why I wouldn’t do them, is that it does not reduce the overlying soft chin pad. Since the chin is a solitary projecting structure any excess is a combination of bone and soft tissue. Reducing only the bone leaves the soft tissue which has very limited to no capability of shrinking down and getting smaller in size. Thus every postoperative symptom you describe is due to the residual soft tissue excess. Only a submental chin pad reduction will be effective now for improvement in both its static and dynamic shape.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I had silicone jaw implants done by another doctor which were subsequently removed during a jaw revision surgery. I have included the original design for your reference. Certain aspects of it, such as the subtle notch, outward gonians, and the ratio of bigonial width to bizygomatic width being 1:1, appealed to me. These implants are what I would like Eppley’s design to be if not better.
Currently I have Medpor implants that are a bit too wide and not as appealing as the initial silicone jaw implant design.
A:Your current extended jaw angle extended implants are about 8mms wide while the ones you prefer are about 3mms wide at most. These differences are in the jaw angle areas primarily, there is not much difference in the anterior extension in either implant design. Since your existing implants are Medpor there are going to be some challenges in their removal, particularly the thinner part of the implant that heads into the chin to merge into the side of the previous bony genioplasty.
Dr. Barry Eppley
World-Renowned Plastic Surgeon
Q: Dr. Eppley, I would like to proceed with the “Special Design Back of Head Skull Implant” option. However, I do have a follow-up question:
How would this pre-designed implant be adjusted to fit the unique shape of my head, considering that it was not created based on my specific CT data? Additionally, would my preferences regarding the shape—which I illustrated during my consultation with Dr. Eppley using the images I shared—still be realized with this option? Finally, is there any risk that the implant might not fit properly?
I apologize for the slight confusion and for asking so many questions, but it is important for me to have more clarity to ensure I am making the best possible decision. I truly appreciate your patience and understanding.
A: The only reasons a patient choses a Special Design (SD) implant is 1) economics (it costs less) and 2) I think what I have available to use will work reasonably well. What counts in any skull implant is the outer contour change, not an intimate fit underneath. Any discrepancy between the implant and the bone will get filled in with scar tissue. The implant sits in place with screws and is stiff enough that it does not flex. What really makes the SD implant possible in your case is the wide open coronal incisional approach where adapting the implant to the shape of the skull can be seen under direct vision. The SD concept does not work as well as when a more traditional ‘blinded’ limited incision approach is used as is done in the vast majority of skull augmentation cases.
That being said the way to obviate any of the SD implant concerns is to just do a true custom design. You choose the SD approach not because it is better but because it lowers the cost of the surgery somewhat.
Dr. Barry Eppley
World-Renowned Plastic Surgeon